
Lisdexamphetamine (Vyvanse) is the new kid on the block and in recent years its use has become rampant among many parts of the population (particularly in the US).
Lisdexamphetamine is a prodrug of dextroamphetamine. Compared to instant-release amphetamine (Adderall), it has a smoother onset and offset, less abuse potential, and slightly fewer side effects. Nonetheless, coming off is just as hard, and (potential) adverse effects on long-term brain health may be the same.
Personal experience
I have tried lisdexamphetamine a couple of times at low doses. Even 10mg (3mg dexamphetamine equivalent) made me overly speedy, though I liked the experience. However, the day after I was always quite tired and “meh”.
Three anecdotes from friends:
Three anecdotes from friends:
- One friend “had the two most productive weeks of his life” before realizing that he was neglecting his basic needs (diet, exercise, sleep, electrolytes) and started to feel like crap. He ended up being off for a couple of months before restarting with a better lifestyle protocol (e.g., setting a timer to eat). A couple of months later, he developed a psychosis (including suicide attempt) that required inpatient treatment. He also smoked a lot of weed during this time, and it is hard to say how much the lisdex contributed.
- Another friend, who is an MD and medical researcher in neurology, tried 20mg of lisdexamphetamine out of curiosity (he usually uses modafinil). According to him, he felt incredibly stimulated like never before but even a single dose led to some listlessness and depressive symptoms for two days after. He also believes that long-time administration of amphetamines in therapeutic doses may be neurotoxic.
- Another friend liked to use pure amphetamine (“speed”) at raves. However, he paid for it with sluggishness and anhedonia lasting for a week or so after. He switched to lisdexamphetamine because he believes it to be “the lesser evil”. He particularly likes the extended-release effect, which enables him to use a lower overall dose to “get him through the night”.
How it works
As discussed in the section on amphetamine, dex-amphetamine has a higher affinity for the dopamine transporter (DAT) and is, therefore, more motivating, while levo-amphetamine has a higher affinity for the noradrenaline transporter (NET) and is, therefore, more physically stimulating.
Lis-dexamphetamine is dex-amphetamine plus the amino acid lysine attached to it. This causes it to be inactive before the lysine side chain is cleaved off by enzymatic action in red blood cells. Red blood cells aren’t capable of metabolizing a lot at a time, so this acts as a natural rate-limiting step in its release, which results in a steady, continuous release of dextroamphetamine into the bloodstream for the next couple of hours.
Its effects generally begin within 1-2 hours and last for up to 14 hours.
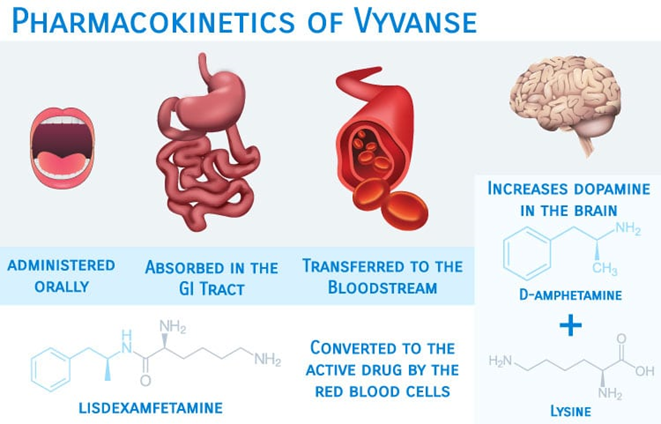
The greatly flattened peak in amphetamine plasma concentrations smooths out the onset and offset. Furthermore, it reduces the associated euphoria and helps to prevent abuse.
After coming off, many people report feeling cognitively, behaviorally, and emotionally blunted. For many, the lethargy and anhedonia get better quickly, but for others, they do not, presumably due to stubborn counterregulatory adaptations on an epigenetic, cellular, and network level.
Speculatively, there may also be a neurotoxic component, especially if lisdexamphetamine had been used at the higher dose range. I discuss the potential neurotoxicity of amphetamines here: Are Amphetamines Neurotoxic?
The antidepressant potential of stimulants
There seems to be a specific pattern of depressive symptoms that is inadequately addressed by serotonergic antidepressants. Among these inadequately addressed symptoms are anhedonia, reduced motivation, loss of interest, fatigue, and apathy.
These “anergic” or “atypical” features of depression are thought to be at least in part due to a relative dopamine deficiency, for which genetics presumably play a large role. Other factors are hormone imbalances, being overweight, and drug abuse, among others.
Unfortunately, conventional antidepressant treatment regimens barbarically neglect the crucial role of dopamine but mainly focus on serotonin and to a lesser degree noradrenaline. This is unfortunate for amotivational and listless types of depression, which are by no means rare.
Treating these patients with SSRIs often exacerbates the issue, causing a state of so-called “amotivational syndrome”, perhaps in part caused by (excess) serotonin further suppressing dopamine signaling.
As described in An Introduction to Neurotransmitters, no matter how much one believes in the importance of psychological factors, dopamine levels are among the primary determinants behind how motivated one is, and how ready one is to push through things to get what one wants.
Besides incentive salience (motivation), dopamine is also important for concentration, zest for life, and the ability to experience pleasure. The philosopher David Pearce argues that dopamine increases the range of activities an animal finds worthwhile pursuing.
And since most antidepressant treatments do not directly enhance DA neurotransmission, this may contribute to “residual symptoms”, including impaired motivation, brain fog, and anhedonia. For many people, these symptoms get better by either switching to a more dopaminergic drug (e.g., from escitalopram to bupropion) or augmenting with one.
The anti-depressive effects of dopamine are twofold.
- Firstly, high dopamine itself “feels good”. Anyone who has ever taken the selective DAT-inhibitor modafinil can probably attest to this.
- Secondly, and more importantly, dopamine increases drive and motivation, which enables people to get up from the coach and improve their life circumstances and themselves. This does not just “feel good” but also has tangible effects in real life, with important bidirectional feedback loops on the psyche.

As psychiatrist Ken Gilman points out, the long-standing neglect of dopamine’s role in depression is reflected in the fact that none of the dopamine reuptake inhibitors (methylphenidate, amphetamine, modafinil) were ever classified as antidepressants (except for amineptine).
It seems that things are slowly beginning to change, and more and more psychiatrists start to use these drugs as augmentation agents (and more rarely, as stand-alone treatments).
So, should everybody simply get on amphetamines? In my opinion, amphetamines should only be used temporarily (if at all), simply because most people tend to be worse off after stopping them. While they are great for treating a lack of volition and related symptoms, the withdrawal is horrible, and the anhedonia and apathy come back with a vengeance. Furthermore, they may have adverse effects on long-term brain health, likely much more than other dopaminergic agents.
Less potent (but more sustainable) substitutes are bupropion, modafinil, and methylphenidate. Low doses of rasagiline or selegiline are also an option, as is testosterone replacement for males. For more severe cases, there is tranylcypromine.
Two “conventional” antidepressants that have an appreciable affinity for the dopamine transporter (DAT) are bupropion and sertraline. While bupropion is classified as a noradrenaline-dopamine-reuptake inhibitor (NDRI), sertraline is wrongly classified (based on pharmacological affinities) as an SSRI – it has more rights to being classified as an “SDRI” compared to venlafaxine as an “SNRI”.

In my opinion, both bupropion and sertraline are suitable first-line antidepressants for depressed individuals with little motivation. Another option is vortioxetine, which has a couple of unique properties. I discuss this in more detail here: What Kind of Antidepressant Should I Choose?
The triple reuptake inhibitors ansofaxine and dasotraline are currently in Phase III and if things go well, both may be available for clinical use in the not-so-distant future. I discuss these molecules in more detail here: Noteworthy Molecules in the Pharmaceutical Pipeline
Sadly, the way modern psychiatry treats depression resembles a strategy to relieve misery instead of promoting well-being. What is lacking from the antidepressant arsenal is a wider range of molecules that enhance dopaminergic or opioidergic signaling.
Both of these neurotransmitter systems are still mostly off-limits, though understandably, as both “feel-good” transmitters carry a non-theoretical risk of causing addiction, particularly in already depressed individuals.
Hopefully, as research progresses (and dogmas abate), psychiatry will eventually be capable of delivering high-functioning and socially responsible well-being.
Other experience reports
For a general discussion of stimulants, and links to accounts of stimulants I have experimented with, click here.
For a full list of experience reports, including non-stimulants, click here.
Other articles on depression
- For a more detailed discussion of depression (and how to treat it): Depression – Causes & Treatment
- Anhedonia, the core symptom of depression, is discussed here.
Sources & further information
- Scientific review: Review of Lisdexamfetamine Dimesylate in Adults With Attention-Deficit/Hyperactivity Disorder
- Anecdotes: Drugs.com – Lisdexamphetamine
- Website: Wikipedia – Lisdexamphetamine
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!