
Methylphenidate (Ritalin) is the prototypical ADHD drug and in most countries (other than the US) it is usually the first-line treatment for ADHD (and/or to “slow down” hyperactive children). Interestingly, about 70-80% of the world’s methylphenidate is consumed by the US.
At therapeutic doses, it increases focus, alertness, and concentration, while decreasing impulsivity. Moreover, due to its potent dopaminergic properties, methylphenidate is an effective (but somewhat underused) augmentation agent in the treatment of depression.
MPD has low oral bioavailability (30-50%) and a duration of action of only about three hours. Therefore, it is often taken in an extended-release form.
I discuss ADHD and my thoughts on it here.
Personal experience
A few years ago, I used low doses of methylphenidate (2.5mg) occasionally as a study aid. I liked that it was short-acting. However, the major drawback was that it improved my focus and alertness at the cost of lateral and creative thinking ability. For example, it was great at studying boring material but very bad for e.g., writing an article.
Furthermore, the counterregulation forced me to use it more frequently, which was an insidious spiral, and I eventually “needed” to use it in order to have a productive study session. In my opinion, taking a low dose once per week is likely fine in a similar way that reaching for coffee once or twice per week is likely fine. However, similar to coffee, it usually escalates quickly.

In my experience, very low doses (1.25-2.5mg) were okay-ish for helping with concentration, alertness, and focus for a couple of hours. Higher doses always made me somewhat “robotic” and worsened my cognition and productivity overall because my brain was overly concentrated, still, and boring. Therefore, for me, MPD was hardly a nootropic but mostly useful for getting boring shit done.
Anecdote time. A colleague of mine took methylphenidate during his university finals to help him concentrate. As he went to the bathroom to wash his sweaty hands, he kept washing for around 30 minutes because he was so focused on the washing aspect. Needless to say, he failed the exam. So much for it being a „cognitive enhancer“.
In sum, methylphenidate is a useful crutch for getting boring things done. Best used very sparingly.
How it works
Methylphenidate is a potent inhibitor of the dopamine transporter (DAT) and the noradrenaline transporter (DAT). Methylphenidate itself is more dopaminergic than noradrenergic (2-3-fold selectivity for DAT over NET), though metabolites differ. Because methylphenidate is a DAT and NET inhibitor, there is some cross-tolerance with other stimulants like modafinil, ephedrine, and amphetamine.
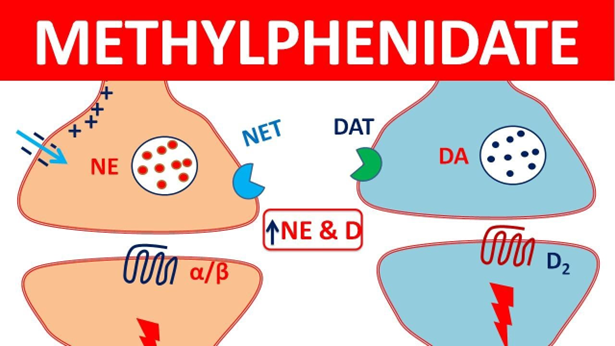
However, unlike amphetamine, methylphenidate does not induce monoamine release. At high doses, releasers such as amphetamine have the potential to increase synaptic cleft monoamine concentration by up to one hundred times, whereas reuptake inhibitors such as methylphenidate elevate monoamine concentrations by up to only about ten times.
Because methylphenidate blocks monoamine reuptake but does not induce release, it is probably less detrimental to long-term brain health than amphetamines, which are potentially neurotoxic (as discussed here). However, a correlation between methylphenidate use and Parkinson’s disease has been found.
From a pharmacodynamic standpoint, methylphenidate and cocaine are quite similar. Both are NET/DAT inhibitors with a greater selectivity for DAT. Both also have a slight affinity for SERT and there are published case reports of serotonin syndrome for both.
However, they are vastly different from a pharmacokinetic standpoint, which changes the user experience completely. Their biggest difference lies in the time they take to peak (crack cocaine > intranasal cocaine > intranasal methylphenidate > oral methylphenidate > extended-release methylphenidate). Nonetheless, because of their similarity, some psychiatrists use methylphenidate to help patients withdraw from cocaine.
Why does methylphenidate “feel” different than amphetamine?
Even though methylphenidate and amphetamine both increase dopamine and noradrenaline, they “feel” quite differently.
Reuptake inhibition, such as with methylphenidate, increases the baseline monoamine concentration in the synaptic cleft but decreases amplitude changes in monoamine concentration that occur between action potentials. In contrast, monoamine releasers have a more neutral effect on amplitude changes, meaning that the change in monoamine concentration in the synaptic cleft between firing and non-firing is normal or large.
Because of this, MPD seems to give people a “glue-like” concentration at higher doses, while amphetamine tends to make people more “speedy”.
Brain changes with long-term use
When children with ADHD are given stimulants for a couple of years, MRI scans show increases in grey matter in specific areas associated with focus and attention and it is hypothesized that these children carry benefits regarding social and cognitive function into adulthood (due to a more “normalized” brain structure). The earlier treatment is started, the more pronounced the effect, for better or for worse.
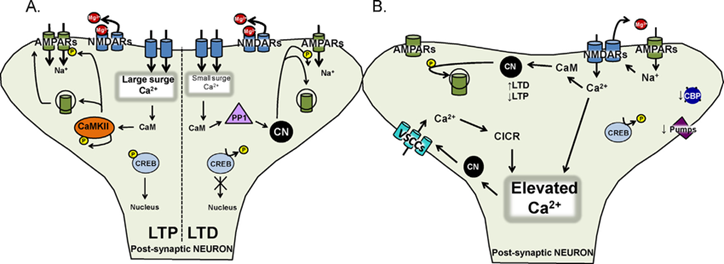
On neuropharmaceutical drugs, certain brain networks and pathways are more active than they would be. As these pathways are used more frequently, the synapses involved are progressively strengthened, also known as long-term potentiation (LTP).
In the case of methylphenidate, pathways involved in selective attention and focus will strengthen, while those involved in creativity may weaken (“use it or lose it”).
I discuss long-term brain changes in more detail here: Why Does Cocaine Make You Cocky and Why Do Psychedelics Make You Weird?
Other experience reports
For a general discussion of stimulants, and links to accounts of stimulants I have experimented with, click here.
For a full list of experience reports, including non-stimulants, click here.
Sources & further information
- Scientific review: Methylphenidate and cocaine: the same effects on gene regulation?
- Scientific review: Methylphenidate Abuse and Psychiatric Side Effects
- Scientific review: The Pharmacology of Amphetamine and Methylphenidate: Relevance to the Neurobiology of Attention-Deficit/Hyperactivity Disorder and Other Psychiatric Comorbidities
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!