
Amphetamine (“Adderall”) is the prototypical stimulant. It was created in the late 1880s and throughout its existence it was – and still is – prescribed for a vast number of conditions, including ADHD, obesity, lethargy, depression, and impulse control disorders such as pathological gambling or binge eating.
Adolf Hitler is thought to have begun using amphetamine occasionally after 1937 and to have become eventually addicted to it in the early 1940s. A vast number of WWII soldiers were using it as well. Were it not for amphetamine, WWII may have perhaps played out quite differently.
At present, millions of individuals diagnosed with ADHD take amphetamines on a daily basis.
Adderall is in a sense similar to anabolic steroids. Online anecdotes tend to paint a “great cheat code for life” picture. However, that picture is very misleading and does not really capture the whole storyline. Lots of cheerleading first-time users who stop documenting their downfall seem to be a common theme.
I discuss lisdexamphetamine (“Vyvanse”), and my personal experience with it, in more detail here.
Personal experience
I have only taken amphetamine a handful of times and only ever at low doses (2-5mg). Even at this dose, it made me restless and speedy. In terms of productivity, I became a demon. As a person, I became unpleasant, insensitive, self-centered, overconfident, and impulsive. It was also hard to relax. As I was still using stimulants, which I now rarely do, I preferred caffeine, modafinil, or ephedrine.

Anecdote time. A friend of a friend of mine used amphetamine to help him build his business. He ended up taking amphetamine daily for 4 years. Despite sleeping poorly, he succeeded in growing his dog supplement business which generates about 100k per year. However, for a variety of reasons, the harm seemed to outweigh the benefits, and he decided to come off.
After quitting, he struggled with mental clarity, depression, anhedonia, and stubborn weight gain. He also had a tough time completing daily tasks. People can tell that “something” happened to him. In the end, he definitely benefited from taking the drug in the short term but was ultimately net harmed by it.
However, I have also met people who seem to tolerate low doses of amphetamines (5-10mg per day) for years on end without seemingly being harmed by them.
How it works
Amphetamine is a substrate as well as a competitive antagonist of the dopamine transporter (DAT) and the noradrenaline transporter (NET). Furthermore, once inside the cell, amphetamine also binds to trace amine-associated receptor 1 (TAAR1), which is thought to cause an efflux of monoamines.
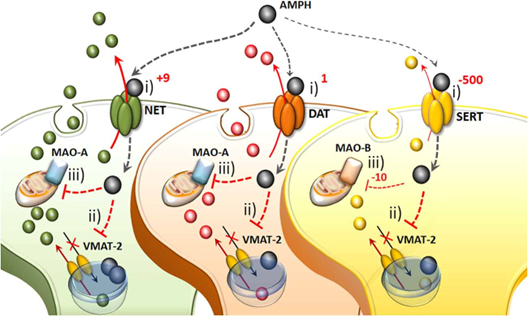
How exactly this efflux occurs – or whether it is an efflux at all – is still a matter of debate. Whatever the mechanism, amphetamine is thought to function as a noradrenaline-dopamine-releasing agent, which seems to be its main mechanism of action.
Through its effects on the noradrenaline system, amphetamine puts the whole central nervous system in a state of intense readiness, which is nootropic and performance-enhancing in itself. In combination with a massive increase in dopamine, this boosts alertness, incentive salience (motivation), task salience, reaction time, cognitive control, and executive function. Furthermore, there is a decreased desire for sleep and food.
The increase in noradrenaline and dopamine boosts prefrontal pathways involved with tasks we call “executive functions”. This makes amphetamines, and their derivatives, a viable treatment for ADHD. At higher doses, amphetamine also causes euphoria, which always happens when dopamine levels rise swiftly. I discuss the noradrenaline and dopamine system, and how to manipulate them pharmacologically, in more detail here.
Its half-life depends on urinary pH levels but is generally around ten hours. The duration of action is around 4-8 hours. Lisdexamphetamine, an extended-release version, is discussed here.
At very high doses, amphetamine can induce psychosis, which is also largely a function of dopamine levels. In fact, given at a high enough dosage and for a long enough time, “amphetamine psychosis” can be reliably induced in pretty much anybody. The symptoms of acute amphetamine psychosis are quite similar to those of the acute phase of paranoid schizophrenia. Furthermore, dopaminergic neurons and related brain networks may change in such a way that psychotic-like states may become recurring events.

A friend of mine, who is a psychosis researcher, uses amphetamine administration as his method of choice to induce psychotic-like states in laboratory animals because, to put it in his words, “amphetamine-psychosis is the only real psychosis”. (He is referring to the fact that drug-induced psychoses from ketamine or psychedelics are neurobiologically different, whereas psychosis from amphetamine mimics the neurobiological aspects of psychosis from schizophrenia much more closely).
The antidepressants bupropion (Wellbutrin) and venlafaxine (Effexor) are both amphetamine derivatives.
Withdrawal
Even though reportedly safe, when amphetamine is administered, there is quite a lot of neurotransmitter depletion and counterregulation. Therefore, letdown effects of deep depression and physical exhaustion often occur. Often, when people take drug holidays, their energy, mood, and motivation vanish into oblivion.
Depending on the dosage and length of use, withdrawal intensity can range from imperceptible to severely debilitating. For some individuals, withdrawal symptoms are short-lived, for others, a protracted withdrawal syndrome may occur, and symptoms are sometimes persisting for months or even years.
This syndrome is thought to be due to persisting physiological adaptations in the central nervous system. This includes disturbances in neurotransmitters, trophic adaptations in brain networks, as well as stubborn changes in gene expression and gene methylation patterns.

The difference between Adderall and Dexedrine
Drugs usually exist in racemic form. That is, as they are synthesized, both mirror images are synthesized in equal amounts, called the “levo”-molecule and the “dextro”-molecule. In some cases, one of the enantiomers is more effective than the other and in other cases, both enantiomers have different effects.
In the case of amphetamine, the enantiomers are L-amphetamine and D-amphetamine (dexamphetamine). L-amphetamine has a greater affinity for the noradrenaline transporter and is, therefore, more noradrenergic, while D-amphetamine has a greater affinity for the dopamine transporter and is, therefore, more dopaminergic. Consequently, L-amphetamine is „pushier“, physically stimulating, and anxiogenic while D-amphetamine feels more motivating and euphoric. The science of dopamine and noradrenaline is discussed here.
Adderall is a combination of different amphetamine salts, totaling about 75% D-amphetamine and 25% L-amphetamine. Dexedrine is 100% pure D-amphetamine.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Fen-Phen
“Fen-phen” is a combination of fenfluramine and phentermine, both of which are amphetamine derivatives. Phentermine is a noradrenaline-dopamine-releasing agent with a NET:DAT ratio of 1:8. Fenfluramine is a serotonin-releasing agent.
Combining these two gives a triple-releasing agent. The “fen-phen” combination was once used as an obesity drug. However, most doctors stopped prescribing it as it was too “aggressive”. Furthermore, it was found that fenfluramine causes valvular heart disease, and fen-phen was quickly withdrawn.
A number of similar obscure stimulants are discussed here: Mighty Molecules Stuck in Pharmaceutical Pipelines
(Ab)Using amphetamines as PEDs
Low doses of dopaminergic stimulants improve athletic performance by a variety of mechanisms. These include improved motivation & alertness, increased power output and reaction time, and a delay in the onset of fatigue.
Furthermore, athletes (ab)use amphetamines to overpower the rising serotonergic tone that occurs upon intense exercise. Whenever mammals exercise intensely (or body temperature gets high), serotonin strongly rises, partially to signal “Hey, you have exerted yourself enough, now chill down.” (Side note: This prolonged rise in serotonin, which is thought to serve self-protective purposes, is also one of the main reasons why intense exercise makes individuals feel good for hours after – as discussed here).
However, when body temperature gets very high, such as it occurs during intense exercise, this rise in serotonin gets so high that it overpowers the dopaminergic and noradrenergic systems putting a break on peak output as a safety mechanism. Dopaminergic stimulants such as amphetamine or modafinil can override this safety mechanism, allowing for a greater and longer peak power output than would otherwise be possible. Therefore, all amphetamines and related molecules are banned by WADA.
Safety
Amphetamines have been used for a long time and are widely regarded as safe.
Anecdotal experience from a large number of people hints at the possibility that long-term amphetamine usage does “something” to the brain, and amphetamines are possibly more neurotoxic than the medical establishment has “evidence” for. I discuss my thoughts on the long-term safety of amphetamines in a separate article here: Are Amphetamines Neurotoxic?
Other experience reports
For a general discussion of stimulants, and links to accounts of stimulants I have experimented with, click here.
For a full list of experience reports, including non-stimulants, click here.
Sources & further information
- Scientific review: Amphetamine, past and present – a pharmacological and clinical perspective
- Website: Wikipedia – Amphetamine
- Scientific review: Toxicity of Amphetamine – An Update (Scientific review: Toxicity of amphetamines: an update
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.