
Large parts of the population in Western countries currently consume either alcohol, cigarettes, weed, toxic amounts of sugar – or a combination of these. Millions of others consume amphetamines, opioids, and cocaine. These drugs provide temporary pleasure, but almost always have negative long-term consequences.
Viewed in terms of mortality, morbidity, or even life enjoyment, people would be better off if they switched to “good drugs”, namely drugs that have long-term beneficial effects on the user. In my opinion, for many bupropion may be such a drug.
Bupropion is a much milder (but much more sustainable) version of amphetamine, of which it is a derivative. It has powerful mood-brightening effects, is stimulating, increases drive, boosts libido, decreases appetite, and, for most people, has few adverse effects once the initial accommodation is over.
Bupropion is an atypical antidepressant that mainly works on the noradrenergic and dopaminergic systems while leaving the serotonergic system mostly untouched.
Bupropion is the only frequently prescribed antidepressant that does not cause weight gain, sedation, or sexual dysfunction – quite the opposite, it tends to improve energy levels & libido and tends to cause weight loss. It also has a milder withdrawal than other antidepressants.
Perhaps unfortunately, bupropion is rarely used as a first-line antidepressant because many physicians assume that it worsens anxiety. Contrary to popular belief, bupropion is no more likely to worsen anxiety than SSRIs, other than perhaps during the first weeks or so (perhaps not at all if one starts it correctly – more on that soon). Furthermore, there is even preliminary evidence that bupropion may be an effective treatment for generalized anxiety disorder and social anxiety disorder (without depression).
For some reason, bupropion is a controlled substance in Russia.
Personal experience
A couple of years ago, I wanted to try out bupropion during a time I felt a little worse than “meh”.

To prevent side effects upon starting, I split the 150mg XL pills into quarters and started with only 37.5mg, increasing the dose by one quarter every three days. Some people assume that the XL pills must not be split because of the pills losing their extended-release effect. However, hydroxybupropion (the major active metabolite) has a half-life of about 20 hours, so splitting them is fine, and particularly at low doses, does not carry an increased risk of seizure.
With this strategy, the initiation was very smooth and pretty much without side effects. Despite the low dose, I felt energized, motivated, and hopeful right from the beginning. Furthermore, bupropion boosted my concentration.
I also stopped drinking coffee so I just switched out one stimulant for another. I also think that bupropion is better (and possibly even healthier) compared to 5 coffees a day, which half of society and most of my colleagues do.
Unexpectedly, it also improved my sleep, as evidenced by my Oura ring. Except for the first two weeks, I didn’t experience any decrease in appetite or increase in libido, both of which are frequently reported by others.
Bupropion helped me to restart old habits and increased my desire to socialize and date. The resulting changes in my inner and outer life killed the “meh”-ness quite quickly.
Despite being a stimulant, it had an overall calming effect on me, likely due to its effect on my concentration. Stimulants can have calming effects on people who are “fast” (therefore their usefulness in ADHD), while they have activating effects on people who are “slow”.
After a couple of months, I increased the dosage to 300mg, but this was too much for me. I love taking long walks and letting my mind wander & wonder. However, on 300mg of bupropion, my mind was disturbingly quiet and devoid of creative or spontaneous output.
Once, I was so fixated on a thought that I nearly stabbed my eye with the scissors I was holding. I quickly decreased the dosage back to 150mg, which was a dosage I liked much better.
Even though bupropion was helpful in many regards, eventually I quit it after about 9 months because it made me subtly “hazy”, absent-minded, and forgetful. I also felt that it worsened my cognition & memory. However, overall, I look back with nostalgia to my time on bupropion, a time during which I rebuilt some aspects of my life in major ways.
A couple of my friends have had great results from it. Two noticed increased anxiety at the beginning, and one noticed a worsened ability to articulate himself, though, for most of them the upsides outweighed the downsides.
However, not everyone does well on bupropion. For example, one of my friends who tried it to help with his seasonal affective disorder felt “high” for three days (bupropion is a substituted cathinone), and then he developed tinnitus. He also could barely sleep for about a week, during which he was bordering on a psychotic-like state. He stopped after about 10 days. Fortunately, the tinnitus went away quickly.
He then reintroduced the bupropion at much lower dosages, ranging from microdoses of 8-20mg per day. According to him, even at this dosage, he liked how the subjective experience of time dilated, which is a function of the increase in noradrenaline levels bupropion causes.
I personally only know one person who felt “nothing different” – everybody else I know who tried it liked it. One psychiatrist I know had been taking 300mg of bupropion for over 20 years.
I returned to bupropion at a later time, about 3 years after my first time on it. This time, my dosage was much smaller. I started with 17.5mg (1/8 of a tablet), stayed there for 2 weeks (a time which I thoroughly enjoyed), and then increased to 37.5mg. After 3 months, for some reason, the feeling of subtle haziness returned and I went cold turkey. However, the 3 months on it were quite enjoyable as well as productive.
All in all, bupropion is a useful antidepressant. I also found it quite useful for life-enriching purposes, at least temporarily.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
How it works
Bupropion is an amphetamine derivative and shares many effects and side effects with other stimulants, such as a reduction of appetite and stimulation of libido. Stimulants are discussed in more detail here.
Similar to other amphetamines, bupropion inhibits the dopamine transporter (DAT) and the noradrenaline transporter (NET) and is therefore classified as a dopamine-noradrenaline reuptake inhibitor (DNRI). Contrary to most other antidepressants, it leaves the serotonergic system mostly untouched.
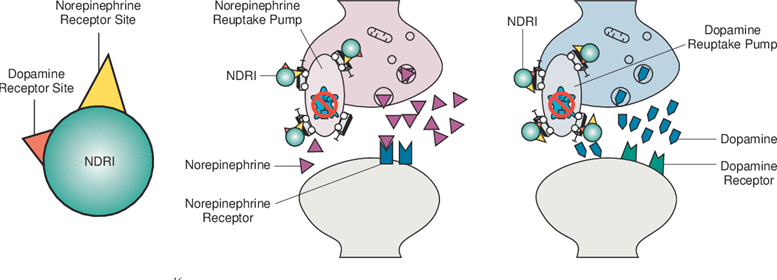
Bupropion itself is quite balanced between dopamine and noradrenaline with a NET:DAT-ratio of about 3:1. However, its major metabolite hydroxybupropion is mostly noradrenergic and only weakly, if at all, dopaminergic. At steady state hydroxybupropion exceeds the concentration of bupropion by about five to ten times. This means, that bupropion increases noradrenaline levels much more than it increases dopamine levels, the exact ratios differ between individuals due to differences in the CYP enzyme system.
At a daily dose of 300mg, the level of DAT occupancy is merely 20%. In contrast, the DAT occupancy with therapeutic doses of methylphenidate or modafinil is about 60%. Given that bupropion is only weakly dopaminergic, how come it increases focus, cognition, and concentration?
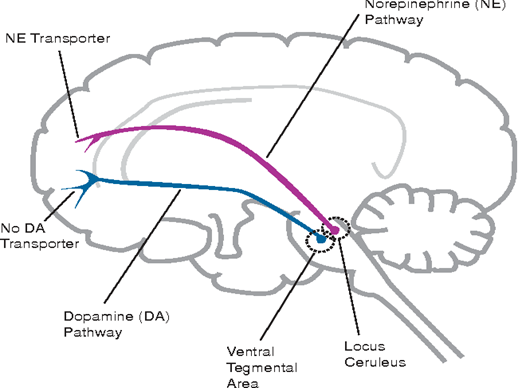
In most of the brain, dopamine reuptake is carried out by DAT, but in the prefrontal cortex DAT expression is very low and most of the dopamine transport is carried out by the noradrenaline transporter (NET).
Therefore, bupropion elevates dopamine effectively in the mesocortical system (where dopamine reuptake happens mostly through NET) but not so much in the mesolimbic system (where dopamine reuptake happens mostly through DAT).
Simplistically speaking, the mesocortical system is responsible for cognition & focus, while the mesolimbic system is responsible for motivation. Both of these pathways are discussed in more detail in the dopamine section in An Introduction to Neurotransmitters.
The metabolism of bupropion is quite variable and depends on an individual’s makeup of the cytochrome P450 system (particularly the CYP2B6 enzyme). The effective doses of bupropion and hydroxybupropion received may differ by as much as five times or so between individuals. Therefore, checking plasma levels for hydroxybupropion seems valuable.
On 150mg/d, my hydroxybupropion levels were only half of the lower end of the reference range for some reason.
If injected or snorted, bupropion causes a “high” like any other dopaminergic drug that peaks fast in the bloodstream. Thus, a reasonable number of amphetamine addicts get bupropion from their doctor, which they then crush and shoot up.
This sometimes results in severe necroses in vascular beds because the extended-release pills are hardly crushable into a fine powder. A psychiatrist friend told me that in the hospital he used to work at, a 30-year-old female lost both of her hands and feet to amputation because of repeatedly injecting poorly crushed bupropion.
Bupropion also modulates a variety of nicotinic receptors. The clinical significance of this in the treatment of depression is unknown, though it is helpful for smoking cessation, for which bupropion is marketed as Zyban. On bupropion, I barely felt the nicotine.
Does bupropion increase anxiety?
It is generally thought that “low serotonin” is involved in anxiety, whereas catecholamines are involved in interest, motivation, and energy levels.
Because bupropion increases noradrenaline levels, it seems logical that bupropion worsens anxiety. However, this is mostly a myth, which even most psychiatrists believe despite ample evidence of the contrary.
Other than in the first week or so, bupropion does not worsen anxiety more than SSRIs and, according to the available data, there is no statistically significant difference in remission rates between SSRIs and bupropion in depressed patients with high levels of anxiety.
Even though the dogma that stimulants make people anxious prevails, for some people the reverse is true, particularly in people with ADHD symptoms. Firstly, the increase in dopamine increases motivation, enthusiasm, and confidence feels good (discussed in more detail here: The Brutal Neglect of Dopamine). Secondly, the increase in noradrenaline levels tends to decrease mind-racing, which lowers anxiety levels for some.

No one I know of who has tried bupropion has experienced anxiety other than during the first couple of days – and only if people take the full tablet right from the get-go just “as the doctor told them to”.
In support of this, there is also preliminary evidence that bupropion may be an effective treatment for generalized anxiety disorder and social anxiety disorder (without concomitant depression).
Usefulness as an antidepressant
Taking psychostimulants for the alleviation of depression is a well-proven strategy. However, in a clinical setting, this is rarely done because of their abuse potential. Bupropion is an exception here.
Because of its weak dopaminergic properties and its flattened peak in the bloodstream, it is hardly abusable in a non-crushed form.
Different kinds of depression are best treated with different monoaminergic drugs. Some researchers speculate that anxious depression is in part characterized by a relative deficiency of serotonin signaling, while anergic or “atypical” depression is characterized by a relative deficiency of catecholamines, especially dopamine (and cortisol).
Whether this is true or not is controversial. Nonetheless, it seems that anxious individuals with poor self-worth fare reasonably well with SSRIs. Conversely, for people with lethargy, anhedonia, and a lack of motivation as their main depressive symptoms, SSRIs often exacerbate the issue, as excess serotonin is thought to reduce dopamine signaling due to inhibitory serotonergic modulation of midbrain dopamine neurons. Therefore, it seems that anergic (“atypical”) individuals fare better with DNRIs, such as bupropion, or MAO inhibitors.
Difference to SSRIs
SSRIs and DNRIs are the most prescribed classes of antidepressants. Currently, bupropion is the only DNRI antidepressant available because methylphenidate and amphetamine are not classified as antidepressants and nomifensine was taken off the market due to an increased risk of hemolytic anemia.
Upsides of SSRIs over DNRIs
- SSRIs are generally more effective in treating anxiety (without concomitant depression).
- SSRIs are generally more effective in individuals with poor self-worth and rejection sensitivity.
- SSRIs are generally more effective at buffering the user against chronic stress.
Upsides of DNRIs over SSRIs
- SSRIs cause some “emotional blunting” (which in many cases is certainly useful) but which is not a “life-enriching” thing to do.
- Some but not all SSRIs tend to cause lethargy, while DNRIs generally increase energy levels.
- Most SSRIs cause an increase in appetite and weight gain, while DNRIs generally decrease appetite and induce weight loss.
- Most SSRIs kill REM sleep, whereas DNRIs generally increase REM sleep.
- SSRIs tend to kill libido, while DNRIs are known to increase it (and are therefore often co-prescribed with SSRIs).
- While most serotonergic antidepressants take about one to two weeks or so to be effective, DNRIs usually start to work somewhat faster. I personally felt bupropion as well as vortioxetine or escitalopram on day 1.
I discuss the different kinds of SSRIs in much more detail here: Thoughts on SSRIs.
Unfortunately, it seems that many doctors know quite little about the difference between the various kinds of antidepressants and tend to give out the same kind of antidepressant to anyone. Most depressed folks are likely to be started on an SSRI – regardless of a patient’s symptomatology.
However, whether a doctor chooses, for example, escitalopram vs. bupropion makes a fairly large difference in how the patient feels and performs for the time the patient is on the drug.
This will eventually have a number of potentially far-reaching 2nd and 3rd-order consequences on many domains of a patient’s life, ranging from work, relationships, sleep, lifestyle choices, and happiness.

A psychiatrist I talked to believes that females in general fare better on SSRIs and males, in general, do better on DNRIs, of which bupropion is currently the only licensed antidepressant. However, I have two female friends who are on bupropion and they both love it.
Potential usefulness as an “anti-addiction” agent
Drugs steal souls. Addicts will often lie, cheat, steal, and cross uncrossable lines to get a fix.
Even “light” addictions can be very disruptive to well-being, productivity, life enjoyment, and society. Substance addiction is widespread, and often, from the outside, other people cannot tell that someone is an addict.
Addiction is not solely an issue of socioeconomically disadvantaged individuals. Modern society is probably full of high-functioning drug addicts and a ton of successful individuals are known to be dependent on a variety of drugs, including amphetamines, benzodiazepines, alcohol, and opioids.

Whatever their background, for many people their addiction is their worst habit. And if people stop their worst habit, every aspect of their inner and outer life tends to make a huge leap forward – and they know it. However, coming off is not so easy, in fact, can be brutal.
Willpower itself is often insufficient. In my opinion, using neuropharmaceuticals wisely is “the lesser evil”. Of the neuropharmaceuticals available, bupropion is perhaps one of the most effective abstinence aids available as it improves well-being, impulse control, attention, energy levels, and motivation.
Other drugs that are potentially useful (and most likely underused) in the treatment of addiction are modafinil, and low-dose naltrexone (LDN). Some people also have success with GLP-1 agonists such as semaglutide, which, anecdotally, does not only reduces food-related cravings but can help with other cravings as well. Some people seem to have (slight) success with N-acetyl-cysteine, which is thought to “normalize” glutamate signaling.
“Harsher” stimulants such as methylphenidate or lisdexamphetamine may be useful as well, though they are somewhat addictive by themselves, so taking them to help with kicking an addiction is essentially switching out one addiction for another (though presumably for a “better” one).
In addition to helping people come off an addiction (whether a behavioral or a chemical one), these agents might also help to prevent a relapse. For example, in the case of bupropion:
- Firstly, it is an effective mood-brightener, stimulant, and antidepressant. Many people relapse when their energy and mood are poor.
- Secondly, and more speculatively, bupropion might help people with creating a life that is fulfilling by itself so that pleasure-short cuts and escapism are not needed anymore.
(Note: When it comes to nicotine addiction, bupropion is extra effective because it is also an antagonist of several nicotinic acetylcholine receptors. When I was taking bupropion, I got very little effects from taking nicotine gum.)
Bupropion helped three friends of mine kick their weed addiction and helped one friend greatly reduce consumption. In my and their opinion, bupropion is the “better” drug. The concept that there are worse and better drugs was introduced in the section Guiding Principles.
In my opinion, using stimulants or antidepressants to help treat (or prevent) addiction is severely underused by modern psychiatry.
Obviously, psychotherapy and other non-biological approaches (e.g., mindfulness training) are potentially helpful as well, though non-biological approaches are beyond the scope of this article. One of the best ways to kick an addiction is probably to change one’s environment. However, radically changing one’s environment is not on the cards for many.
A “mix” between a biological and non-biological approach is psychedelic therapy. While the agents mentioned above reduce craving from a neurobiological side, psychedelics may address the psychological side of things. Essentially, psychedelics can be compared to “months’ worth of psychotherapy in a single afternoon”. Anecdotally, the atypical psychedelic ibogaine seems to be extra effective for opioid or cocaine addiction.
I agree with philosopher and neuropharmacology enthusiast David Pearce: “In most cases, the issue amounts not to drugs vs. no drugs, but rather to allow people to opt for better ones. However perversely, the more useful the drug, the harder it is to usually get hold of in our modern society.”
Unfortunately, for many readers assault rifles are easier to get hold of than most of the molecules discussed on this website.
Other
In combination with dextromethorphan, bupropion is now available as a new antidepressant called Auvelity. Supposedly, Auvelity was specifically designed to help people with anhedonia.
In combination with naltrexone, bupropion is available as the formerly popular weight-loss drug (Contrave), which though is now effectively being driven off the market by GLP-1 agonists, such as semaglutide.
Other experience reports
For a general discussion of stimulants, and links to accounts of stimulants I have experimented with, click here.
For a full list of experience reports, including non-stimulants, click here.
Sources & further information
- Anecdotes: Reddit – r/bupropion
- Scientific review: Bupropion for attention deficit hyperactivity disorder (ADHD) in adults
- Opinion article: Psychiatric Times – Three Myths About Bupropion
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.