
A good friend of mine has recurrent episodes of depression. Whenever depression is looming, he feels hopeless and helpless. Even though he knows exactly what is happening (he is a doctor), what he feels takes over. According to him, a single injection of ketamine is the only thing that reliably gets him out before the depression gets worse.
Ketamine has been used for anesthetic purposes since the 1970s. For recreational purposes, “Special K” is abused throughout the world, especially in Southeast Asia and the UK. However, at lower than anesthetic or recreational doses, ketamine has some unique and interesting properties.
Currently, in psychiatric wards all over the world, there is a lot of talk and hype about using ketamine to treat a variety of conditions, especially deep biological depression. Taken at around 1/10th of an anesthetic dose, it rapidly lifts mood, abolishes suicidal thoughts, bans anxiety, and even improves obsessive-compulsive symptoms – at least for a subset of patients.
Compared to other drugs, ketamine exerts its effects not until after the drug has already left the system. Furthermore, the effects are “natural”, in the sense that the balance of monoamine neurotransmitters is not distorted.
While single-use ketamine is known to improve well-being, energy levels, and cognition for about 1-2 weeks (and more rarely months), repeated-use ketamine, a so-called “ketamine series”, is thought to bring about powerful neuroplastic changes.
The main benefit of ketamine is a rapid reduction in depressive symptoms, particularly suicidal ideation. The main problem with ketamine is that the benefits are mostly transient (at least for most people) and the potential neurotoxicity, which may already occur at therapeutic doses.
Personal experience
Once upon a time, a friend asked me to join him in doing ketamine, which he occasionally does for spiritual reasons. I had long been curious about it – especially whether it had any effects on me as a non-depressed person.
I took the standard psychiatric dose (0.5mg/kg).
We were in a pitch-black room with little sensory input. I did not particularly like the experience. In fact, I found it to be quite scary. It seemed that all matter had dissolved and there was just consciousness left.
Initially, I thought I had killed myself. Then, a lot of scenes and images of my friends & family appeared in rapid succession before my closed eyes. Never before had I had such vivid hallucinations, not even with psychedelics. I was reflecting a lot on my life, and I had a couple of interesting insights.
Even though my mind was crystal clear and my thinking lucid, this was unlike anything I had ever experienced. It was definitely “weird”.
The next day I did not think much of it, and I felt a little off, perhaps as we did the ketamine in the evening, and the associated cortisol spike then hampered my sleep.
The morning thereafter, around 36 hours after taking the drug, I was on the subway listening to music. I remember it to this day. It suddenly occurred to me that I was moved to tears by a sappy love song. For the next 10-14 days, I felt like I did during puberty. Full of energy and emotions, which I thoroughly enjoyed. This was definitely mild hypomania. Thereafter, my baseline emotionality was still elevated.
During all this time, I had also been more present and motivated, and I had barely used any stimulants, simply because I did not need them.
I was intrigued.
After two weeks, I repeated the experiment. The ketamine experience itself was again somewhat “weird”, though much less scary than the first time. The post-experience increase in emotionality, sharpness, and zest was undeniable.
After two more sessions, each separated by about two weeks, I decided to continue because I find that life is much richer if my emotions are intense and deep. And my nervous system’s ability to generate intense emotions depends on its neurobiology, which ketamine seemed to alter in a way I liked.
I found that if I moved my ketamine sessions much earlier in the day, I do not feel “off” the day after. I also started to enjoy the sessions – perhaps a little too much.
One hour per week to make the whole week better? I take it.
I continued doing this for about six months at the same dosage and frequency. Initially, the after-effects were strong and in the following days everything seemed a little crisper, and my energy, mood, and “punch” were all noticeably increased. Furthermore, I could feel all sorts of emotions – even subtle social emotions I do not normally feel. In contrast to the other antidepressants I had tried, such as moclobemide, vortioxetine, or bupropion, ketamine did not remove negative emotions, which is something I liked.
Unfortunately, even though I waited 1-2 weeks between doses, after some time the effects vanished drastically to the point of being gone almost completely. Each time the response got somewhat weaker and more short-lived. Not just the vivid imagery during my experiences, but also the desired after-effects. So much so that after about six months, the strength was only about one-third to one-fourth compared to my first session, if at all.
I disclosed my ketamine use to two friends who are psychiatrists, and both believe that ketamine is neurotoxic even at therapeutic doses and frequencies. Furthermore, both human and animal data confirm the neurotoxicity of ketamine. Because of the real risk of neurotoxicity, I stopped taking it.
Upon retrying ketamine a year later, about 24 hours after administration I felt a distinct increase in “presence”, enhanced emotions, and great energy and mood. My mind just felt more “awake”. Based on preliminary research, I took 5mg of everolimus 2h beforehand hoping that mTOR-inhibition extends the duration of action and also reduces some of the (potential) neurotoxicity. The ketamine-induced boost in energy and mood lasted about 10-14 days, after which it subsided (almost?) completely.
In sum, other than with MAO-inhibitors of psychedelics, the best I’ve felt in my twenties (from a biological perspective) was during the first few days after my initial experiences with ketamine. I had boundless energy, crisp mental clarity, and was low-level euphoric for a couple of days – despite not having been depressed in a way I could tell, as I do not have obvious issues with mood or motivation that go beyond what “normal” people experience.
Does this say about me that I have a form of (neurobiological) high-functioning depression? Or does ketamine make a subset of non-depressed people feel & function better? I am not sure. Some of my friends are similar to me in that they have an undeniable increase in vitality the days after ketamine, whereas others do not feel any different.
One friend had success with ketamine after a COVID-19 infection, which left him feeling lethargic and semi-depressed for about a month. Shortly after taking a single low-dose ketamine, he was back to baseline and the effects presumably carried him through until the after-effects of the infection had naturally subsided. It is also part of my Long-COVID prevention protocol, as described here.
One thing that possibly makes ketamine a little less neurotoxic, is taking 1800mg of N-acetyl-cysteine a couple of hours before. NAC reduces the generation of reactive oxygen species, which may help a little.
My current use of ketamine
From time to time, I struggle with anhedonic depression. This happens about 1-3x per year lasting a couple of weeks. I had been dealing with this for years now. During these episodes, I do all the things I normally do (e.g., work, gym, friends) but I feel quite little. The weird thing is that from the outside nobody can tell.
When I tell friends that during these times I actually feel quite a little, they usually do have a hard time believing me because I am laughing, making jokes, and seeming just like always. I am not even acting or putting up a facade. I am also not dissociated. There is just a mismatch between what I do and what I feel. Even my psychotherapist does not believe me (“A person that feels little is not acting and talking the way you do.”). However, on the inside, there is emptiness. It is quite hard to explain.
Also, these episodes seem to have very little effect on my “objective” life. I still go for walks, reading, dating, and my ambition is barely affected. However, I do all of these things without “feeling” much. Other than the anhedonia, I am also more fatigued and sometimes it is a drag to schlep myself through my days. I am quite sure the cause is biological and not psychological.
I hypothesize that during these times neuroplasticity is at low levels as I barely ever dream. Anyway, a single dose of ketamine has thus far always been sufficient to kick me out of it.
I am always reluctant for a couple of weeks to use it because it is probably more neurotoxic than the medical community currently appreciates. If the “waiting it out” does not work, I use ketamine.
For the first day, I feel not much – perhaps a little woozy. About 24 hours after, there is a 1-2 hour ramp-up period during which I start to feel more “awake” (hard to explain) and it seems as if somebody had turned on HD vision (or more likely, removed a “veil” that had been present). I usually feel very good, am present in the moment, I have deep emotions, I can work for many hours on cognitively demanding tasks, my sleep needs decrease, and my libido rises. Sometimes, I think ketamine triggers a short-lived period (a couple of days) of hypomania – or normalcy?
Often, my feelings remain turned on for a few days, sometimes for a few weeks, and sometimes even for months. I aim to not use it more often than once a quarter (ideally, less).
Recently, I also found NSI-189 very valuable in terms of getting out of this state. Since gaining weight (both body fat as well as muscle) and hopping on the HCG I only got one (plus one minor) of these episodes. This article was mostly written in early 2024. At the time of editing and publishing it (12/25), I have not got a single one of these episodes for a whole year – knock on wood and Iast year I only used ketamine once – prophylactically as part of my Anti-LongCOVID protocol.
How it works
There are two major competing theories about how ketamine may work.
Theory #1
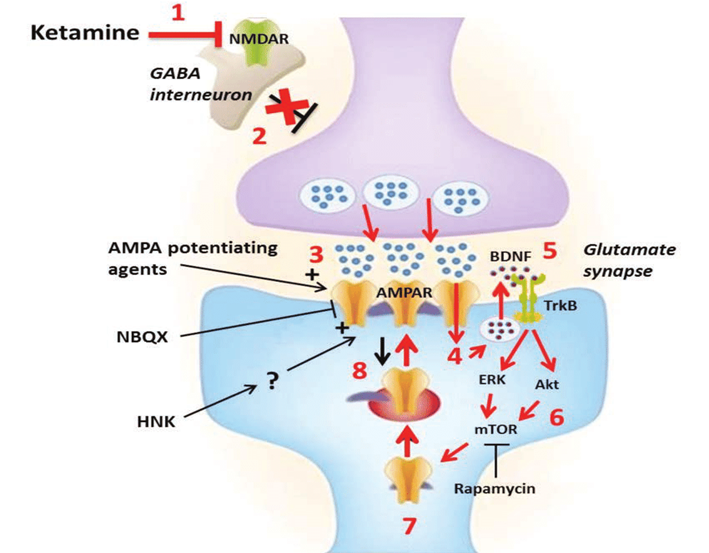
Ketamine blocks the NMDA receptor (a glutamate ion channel), which is among the most important receptors involved in synaptic long-term potentiation. Blocking this receptor leads to a glutamate rebound, which then leads to potent AMPA receptor activation, the major excitatory glutamate receptor.
The subsequent burst in AMPA signaling, modulates a number of downstream signaling pathways, including activation of mTOR, and the expression of a host of nerve growth factors such as BDNF or VEGF.
These growth factors then promote neurogenesis & synaptogenesis, and lead to a general increase in glutamate signaling throughout the nervous system. The neurogenesis plus the increase in glutamatergic neurotransmission are then thought to exert ketamine’s therapeutic effects.
Theory 2
Some researchers believe that ketamine’s action at the NMDA receptor is irrelevant, given that memantine, another NMDA receptor antagonist, does not have antidepressant effects. These researchers believe that all or most of ketamine’s antidepressant effects come from its metabolite hydroxynorketamine, which is thought to induce sustained activation of the AMPA receptor but lacks any appreciable affinity for the NMDA-receptor, acting as a so-called AMPAkine (discussed in more detail in the article on racetams). Hydroxynorketamine is currently in Phase I for the treatment of MDD. This theory has fallen largely out of favor.
Whatever the mechanism, racemic ketamine has seemingly magical effects when it comes to helping people with deep “biological” depression. While some people might not respond at all, others feel well, sometimes for the first time in their life.
The antidepressant effects of ketamine are thought to be due to two independent mechanisms:
- The acute mood elevation (hours) of ketamine may stem from its affinity to the mu-opioid receptor, which is activated by opiates such as heroin, oxycodone, and fentanyl. Co-administration of naltrexone is known to block this immediate mood boost. Ketamine’s affinity for the mu-opioid receptor is also thought to be the major reason why ketamine is pleasurable and addictive, especially at higher doses.
- The sustained mood elevation (days) is thought to be due to the upregulation in growth factors (e.g., BDNF, VEGF) as well as a prolonged uptick in glutamate signaling. These last for about one to two weeks, about as long as the antidepressant effects of ketamine do. There are preliminary data that a single dose high dose of rapamycin before ketamine can prolong the antidepressant effects of ketamine, speculatively due to the suppression of microglia cells, which are prevented from gobbling up the newly created synapses.
The duration of the response can vary widely from no effect at all to a single administration having beneficial effects for over 30 days. Most people seem to experience benefits ranging from 7-14 days.
A series of ketamine administrations within a short time span (e.g., 4-6 administrations within a 3–4-week period) is, in select cases, able to produce remission of depression for many months – presumably because of the intense boost in neuroplasticity.
I believe that if ketamine were not (potentially) neurotoxic, it may be the ideal therapy for a certain kind of neurobiological depression (which is not the same as “suffering”).
- Firstly, it does not “distort” neurotransmitters in the same way reuptake inhibitors do.
- Secondly, instead of blunting emotions like pretty much every other antidepressant (perhaps with the exception of bupropion or MAO-inhibitors) it enhances emotions and many people report that the days after ketamine they are able to feel feelings again.
- Thirdly, it does not need to be taken every day and sometimes the frequency of administration can be as low as once per month.
Environmental enrichment “in a pill”?
On a molecular level, some of the antidepressant effects of psychedelics are somewhat similar to ketamine. Both ketamine and psychedelics mediate an increase in both structural as well as functional plasticity (e.g., neuritogenesis, spinogenesis) that presumably follows similar molecular mechanisms (e.g., activation of TrkB and mTOR), both in vitro as well as in vivo.
In the modern world, most people like to stay in their houses and are therefore exposed to little “environmental enrichment”. Environmental enrichment has potent anti-depressive effects in part because it boosts synaptogenesis.
This is one of the many reasons why people feel much less depressed if they travel. Repeated ketamine use (or psychedelic use) may potentially deliver environmental-enrichment-stimulated neurogenesis artificially.

A psychiatrist I worked with used to say that millions of people need ketamine particularly because of this reason, namely that they lack environmental enrichment. However, serious concerns about addiction and neurotoxicity remain (discussed shortly).
Anhedonia
All antidepressants I have tried so far (e.g., vortioxetine, moclobemide, bupropion) blunted my emotions to some extent (with the exception of low doses of tranylcypromine). One of the few things that did not, but instead enhanced my emotions, was ketamine. Ketamine is an effective treatment for anhedonia, the core symptom of depression. Anhedonia is a difficult beast. I discuss it, and a couple of potential ways to treat it, in more detail here: Anhedonia
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Safety – Ketamine is probably more neurotoxic than you think
It is clear that ketamine at a sufficient dose & frequency can and does kill neurons through NMDA-driven excitotoxicity. However, what does a sufficient dose & frequency mean?
There is a common myth that ketamine is “neurogenetic”. This is mostly false. While it does increase neurogenesis in the only two places in the brain where neurogenesis happens (the hippocampus & subventricular zone), for the rest of the brain it only increases neuroplasticity. However, while local neurogenesis and neuroplasticity increase temporarily, ketamine also kills neurons diffusely throughout the brain, which is irreversible. In fact, dozens of animal studies – and human observational studies – unequivocally show that ketamine is neurotoxic – at least at high dosages.
The search term “ketamine neurotoxicity” gives over 400 results on PubMed and there is lots of conflicting evidence.
At recreational doses, ketamine is addictive, destroys the bladder, and is toxic to the central nervous system. Microscopic lesions (including but not limited to so-called “Olney’s lesions”) in both grey and white matter are evident already after three months of high-dose ketamine use.
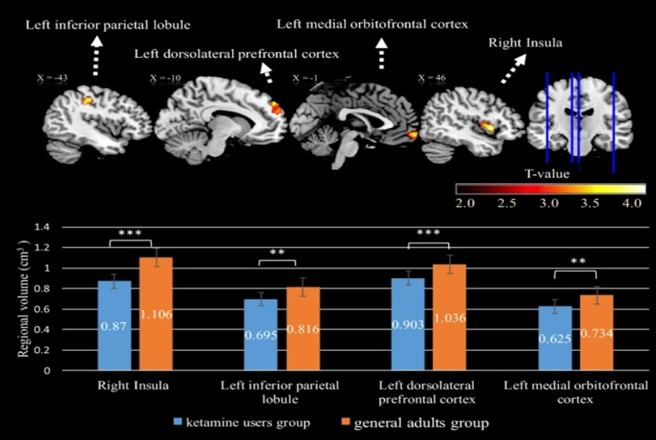
By year three of heavy use, MRI scans of ketamine users often reveal a profoundly degenerated brain featuring white matter degeneration, cortical thinning, and grey matter atrophy.
If ketamine were truly neurogenetic, we would find a grey matter increase – however, we always find the opposite – atrophy.
Ketamine abuse is well known to cause widespread cognitive and neurological impairment – and shockingly fast too (months to years). However, a heavy ketamine “user” often consumes multiple grams per week, which is a lot more than therapeutic use (0.5mg/kg about once per week to every other week). One glass of wine per week is surely different from a gallon of vodka per day.
However, visible brain damage (MRI) has been described in the literature already in users who use much less. The lowest I could find was someone who used about 200mg twice per week for six months. With a bioavailability of about 50% for intranasal consumption, this would be a little less than 2mg/kg – about 4 times the commonly used therapeutic dose (0.5mg/kg), and about an average party dose. In this user, slight changes to grey and white matter were already evident 6 months after starting (source). The observed changes included “holes” (degenerative white matter patches) as well as visible cortical lesions and atrophy. Obviously, the observation of drug users has a lot of confounders (e.g., undisclosed polytoxicomania). Nonetheless, I find this concerning.
It should be noted, that early forms of brain damage are microscopic and cannot be picked up by currently available imaging technologies, so if something is visible, it is quite advanced.
Furthermore, individuals who occasionally use ketamine find they need significantly higher doses than when they first started, even after prolonged periods of abstinence. For instance, after a few months of using therapeutic doses of ketamine (around 0.5mg/kg per week), I noticed that its impact was much less pronounced compared to my initial experiences with the substance. Even extended breaks did not bring back my virgin response – in an analogous way that MDMA users never recapture the magic of their first few trips. This form of “permatolerance” may point to neurotoxicity – in the same (but mechanistically different) way it does with MDMA.
I looked into this matter quite extensively because I occasionally suffer from anhedonic depression and, rarely, I use therapeutic ketamine injections (discussed in more detail here). I talked to a handful of university psychiatrists who have been using ketamine on some of their patients for years – long before Spravato (esketamine nasal spray) was available. Every single one of them believes that ketamine is at least somewhat neurotoxic but is the lesser evil if contrasted to otherwise untreatable depression.
Furthermore, depression itself is quite damaging to brain health and it is very likely that long-term administration of neuropharmaceuticals (e.g., stimulants or antidepressants) has effects on the brain as well. Thus, the risks and side effects need to be weighed against the risks and side effects of alternatives.
It is currently unclear whether ketamine at low therapeutic doses at reasonable frequencies is neurotoxic. Mainly because slight brain damage will be neither picked up by clinical tests nor currently available imaging technologies – however, the absence of evidence is not evidence of absence and it is possible, perhaps even plausible that regular low-dose ketamine administration is low-level neurotoxic and that very subtle changes could accumulate over the years.
On r/therapeuticketamine there is the occasional person complaining about memory loss, particularly the ones that are being administered high doses quite frequently. But again, anecdotes are anecdotes.
There is one study that looked at ketamine administration long-term and did not find evidence of neurocognitive decline. However, they were using clinical tests, which are not very sensitive and to reach statistical significance quite a bit of deterioration would need to happen. Depressed individuals often have brain fog, rumination, memory problems, and poor thinking abilities (dubbed “depressive pseudodementia”). So, if someone goes from depressed to non-depressed, and stays non-depressed for quite some time, should cognition not improve? In other words, if ketamine effectively treated their depression (which it reportedly did), should there not be an increase in cognition between baseline and timepoint X? Did neurocognitive domains indeed improve but the improvement was then masked (or erased) by gradual neurotoxicity?
In sum, we can say that ketamine used at “party doses” is almost certainly neurotoxic but the jury is still out on whether ketamine at therapeutic doses is or not.
Mechanism of neurotoxicity
There are multiple potential mechanisms. The most likely mechanism is the following. NMDA receptor blockade leads to an increase in extracellular glutamate, which then activates AMPA receptors in excessive amounts. The excessive AMPA receptor activation then leads to a sharp influx of calcium, which then kills neurons by excessive excitation (excitotoxicity) through both apoptosis and necrosis. This excitotoxicity most likely happens during the ketamine high.
Supplements such as N-acetyl-cysteine may help to counteract it to a small degree. Coadministration of benzodiazepines can prevent some of the excitotoxicity – but unfortunately also part of the therapeutic effects.
Psychedelics and ketamine trigger some of the same intracellular signaling pathways (e.g., BDNF -> TrkB -> mTOR). Like ketamine, psychedelics trigger an increase in neuroplasticity (spinogenesis and synaptogenesis) but they are not known to be neurotoxic. Unfortunately, psychedelics can occasionally cause HPPD, which can, in severe cases, be incredibly distressing.
But isn’t ketamine neurogenetic?!
What most people mean when they say something increases neurogenesis, they mostly mean it increases neuroplasticity, which, for practical purposes is limited to the generation of dendritic spines (spinogenesis) and synapses (synaptogenesis). Spinogenesis and synaptogenesis are very different from neurogenesis (the birth of new neurons). Neurogenesis is limited to two sites in the human brain (the hippocampus and the subventricular zone) and a local creation of neurons in these sites cannot make up for the death of functionally integrated neurons elsewhere. So, ketamine increases neurogenesis in two small brain sites (like most other antidepressants) and it also increases neuroplasticity (at least for a couple of days).
Local neurogenesis plus synaptogenesis & spinogenesis are reversible and usually short-lived (weeks) but dead neurons will never undie.
Given that Spravato (esketamine nasal spray) has been widely available and so-called “ketamine-clinics” proliferated, we are possibly going to have an answer to the question regarding whether and the extent of ketamine neurotoxicity soon. In the meantime, it is probably prudent to err on the side of caution.
My gut feeling is that people who are doing ketamine at even therapeutic doses regularly are more likely than not to give themselves non-negligible amounts of irreversible brain damage.
Unfortunately, ketamine has become a frequent drug of abuse at doses far higher than therapeutic doses. Similar to MDMA (although by a completely different mechanism), the neurotoxicity caused by high doses is irreversible. It is also quite worrying to see ketamine clinics mushrooming everywhere, with some patients reportedly going in twice per week and being given infusions of 100mg or more, which, considering the doubled bioavailability compared to inflation, is definitely in the “party dose” territory. As so often, hype and industry are about to destroy something that was originally quite useful in select cases.
Which form of ketamine is best?
In my opinion, the hype around esketamine is a marketing ploy. Racemic ketamine is cheap as dirt and has been around for about 50 years.
To make a lot of money, big pharma pursued esketamine, even though clinical experience and experimental evidence favored the racemic version, which however cannot be patented anymore. For the pharmaceutical industry, the patent is everything.

I predict that once the patent on esketamine expires, big pharma will go after arketamine and patent that.
Arketamine is significantly weaker, by about eight times, at the NMDA receptor and the dopamine transporter (DAT). However, it is significantly more potent at activating the sigma receptor and AMPA receptor subtypes.
Perhaps more importantly, both enantiomers lead to the formation of hydroxynorketamines, which may explain part of ketamine’s therapeutic effect.
Given that we still do not fully understand by what mechanism ketamine leads to potent antidepressant effects, the best bet is probably to go for the racemic mixture.
How I would do ketamine therapy
How to properly do ketamine therapy is not well established, in part because it seems to depend somewhat on the individual. The most commonly used starting dose is 0.5mg/kg (IV or i.m.).
The widely held belief that “only IV ketamine works” is a myth. The only upside of doing ketamine intravenously is a flattened and reduced intensity of ketamine’s psychomimetic effects, which might be troublesome for troubled minds. If dosage and purity are controlled for, a neuron does not care how ketamine made its way into the bloodstream.
In my opinion, intramuscular or subcutaneous injection is the best route of administration.
Anecdotally, some people notice a clearance of depression and brain fog immediately after their first session, which is thought to be in part related to an improvement in glutamate signaling, or possibly due to its affinity for mu-opioid receptors.
Rarely, a single dose can have effects for well over a month but, for most people, the effects from a single dose last about 5-10 days (given that the individual is a responder to ketamine in the first place).
Usually, ketamine is done more frequently in the beginning (e.g., every 3-7 days) although more frequent dosing is associated with adverse effects, especially depersonalization and derealization.
If I were to do a ketamine series, it would look like this:
- I would start with an initial dose of 0.5mg/kg (SC or IM bolus injection).
- I would repeat this about once a week, sooner if ketamine did nothing, and later if there are still benefits at the 7-day mark.
- If there is no undeniable benefit after 3 doses, I would discontinue.
- If there is benefit, would continue doing this for about 6 weeks and I would use the lowest dose and frequency possible to reduce the risk of incurring (potential) neurotoxicity.
- After that, the repeated doses of ketamine may have resulted in enough neuro/synaptogenesis that dosing can be spread even more, for example, about once per month.
- If ketamine loses its efficacy, I would not increase the dose or frequency as ketamine in high doses or frequencies may be irreversibly neurotoxic. Rather, I would take an extended break. If ketamine ceases to work even after an extended break, I would stop.
- I would never do ketamine in recreational doses. Even single high-dose use may have non-negligible neurotoxic effects, which are neither evident to the user nor to doctors.
A lot of ketamine clinics are giving out 3-6 doses even if the patient does not experience any benefit. In my opinion, this is mostly done to make money and not to help the patient. Psychiatrists who are not financially incentivized to overdo ketamine told me that responders usually respond to the first, or sometimes second and more rarely third infusion – and if they have not responded early, it is highly likely that they do not respond at all.
Other
Ketamine is similar to dextromethorphan (DXM), which is, like ketamine, an antagonist at the NMDA receptor as well as an agonist at the sigma receptor. Dextromethorphan has recently become available in combination with bupropion for the treatment of anhedonia (Auvelity). Anecdotally, DXM is particularly effective in treating anhedonia – at least in the short term.
Ketamine as an anti-withdrawal agent
For the past 2 years, I withdrew a number of drugs. Among them are thyroid hormones, semaglutide, and moclobemide. Usually, coming off anything that interferes with neurobiochemistry is quite unpleasant. For example, coming off thyroid hormones in the past made me feel tired and semi-depressed for at least a week. Coming off semaglutide and moclobemide was similar – mostly extended tiredness.
I found that if I use a very low dose of ketamine (20-25mg), I can come off things in a cold-turkey way and have no withdrawal whatsoever, because the ketamine kicks me into a temporary hypomania-like state (usually lasting for roughly a week or so), useful to bridge the withdrawal.
The major downside is that ketamine is potentially neurotoxic – definitely present at higher doses, and probably also at lower doses. I discuss its neurotoxicity here.
Other experience reports
For a discussion of the molecular correlates of well-being, and links to accounts of various related molecules I have experimented with, read here.
For a full list of experience reports click here.
Sources & further reading
- Anecdotes: Reddit – r/therapeuticketamine
- Scientific review: Ketamine and depression: a narrative review
- Scientific study: Antianhedonic Effect of Repeated Ketamine Infusions in Patients With Treatment Resistant Depression
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.