
It is clear that ketamine at a sufficient dose & frequency can and does kill neurons through NMDA-driven excitotoxicity. However, what does a sufficient dose & frequency mean?
There is a common myth that ketamine is “neurogenetic”. This is mostly false. While it does increase neurogenesis in the only two places in the brain where neurogenesis happens (the hippocampus & subventricular zone), for the rest of the brain it only increases neuroplasticity. However, while local neurogenesis and neuroplasticity increase temporarily, ketamine also kills neurons diffusely throughout the brain, which is irreversible. In fact, dozens of animal studies – and human observational studies – unequivocally show that ketamine is neurotoxic – at least at high dosages.
The search term “ketamine neurotoxicity” gives over 400 results on PubMed and there is lots of conflicting evidence.
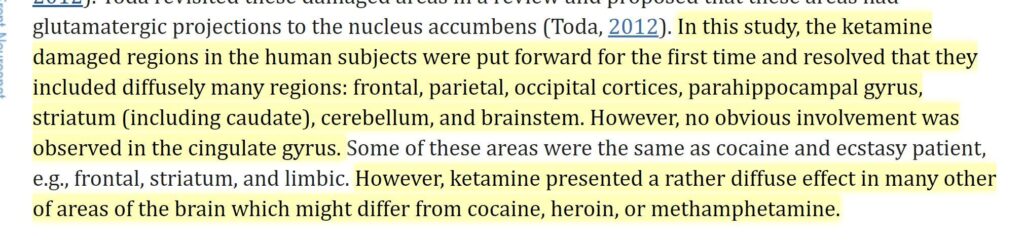
At recreational doses, ketamine is addictive, destroys the bladder, and is toxic to the central nervous system. Microscopic lesions (including but not limited to so-called “Olney’s lesions”) in both grey and white matter are evident already after three months of high-dose ketamine use.
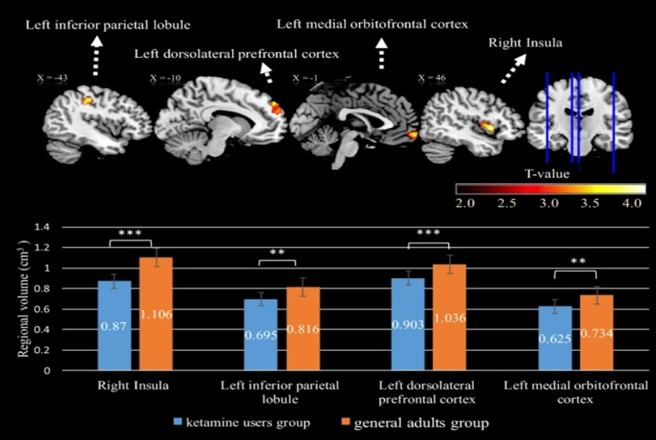
By year three of heavy use, MRI scans of ketamine users often reveal a profoundly degenerated brain featuring white matter degeneration, cortical thinning, and grey matter atrophy.
If ketamine were truly neurogenetic, we would find a grey matter increase – however, we always find the opposite – atrophy.
Ketamine abuse is well known to cause widespread cognitive and neurological impairment – and shockingly fast too (months to years). However, a heavy ketamine “user” often consumes multiple grams per week, which is a lot more than therapeutic use (0.5mg/kg about once per week to every other week). One glass of wine per week is surely different from a gallon of vodka per day.
However, visible brain damage (MRI) has been described in the literature already in users who use much less. The lowest I could find was someone who used about 200mg twice per week for six months. With a bioavailability of about 50% for intranasal consumption, this would be a little less than 2mg/kg – about 4 times the commonly used therapeutic dose (0.5mg/kg), and about an average party dose. In this user, slight changes to grey and white matter were already evident 6 months after starting (source). The observed changes included “holes” (degenerative white matter patches) as well as visible cortical lesions and atrophy. Obviously, the observation of drug users has a lot of confounders (e.g., undisclosed polytoxicomania). Nonetheless, I find this concerning.
It should be noted, that early forms of brain damage are microscopic and cannot be picked up by currently available imaging technologies, so if something is visible, it is quite advanced.
Furthermore, individuals who occasionally use ketamine find they need significantly higher doses than when they first started, even after prolonged periods of abstinence. For instance, after a few months of using therapeutic doses of ketamine (around 0.5mg/kg per week), I noticed that its impact was much less pronounced compared to my initial experiences with the substance. Even extended breaks did not bring back my virgin response – in an analogous way that MDMA users never recapture the magic of their first few trips. This form of “permatolerance” may point to neurotoxicity – in the same (but mechanistically different) way it does with MDMA.
I looked into this matter quite extensively because I occasionally suffer from anhedonic depression and, rarely, I use therapeutic ketamine injections (discussed in more detail here). I talked to a handful of university psychiatrists who have been using ketamine on some of their patients for years – long before Spravato (esketamine nasal spray) was available. Every single one of them believes that ketamine is at least somewhat neurotoxic but is the lesser evil if contrasted to otherwise untreatable depression.
Furthermore, depression itself is quite damaging to brain health and it is very likely that long-term administration of neuropharmaceuticals (e.g., stimulants or antidepressants) has effects on the brain as well. Thus, the risks and side effects need to be weighed against the risks and side effects of alternatives.
It is currently unclear whether ketamine at low therapeutic doses at reasonable frequencies is neurotoxic. Mainly because slight brain damage will be neither picked up by clinical tests nor currently available imaging technologies – however, the absence of evidence is not evidence of absence and it is possible, perhaps even plausible that regular low-dose ketamine administration is low-level neurotoxic and that very subtle changes could accumulate over the years.
On r/therapeuticketamine there is the occasional person complaining about memory loss, particularly the ones that are being administered high doses quite frequently. But again, anecdotes are anecdotes.
There is one study that looked at ketamine administration long-term and did not find evidence of neurocognitive decline. However, they were using clinical tests, which are not very sensitive and to reach statistical significance quite a bit of deterioration would need to happen. Depressed individuals often have brain fog, rumination, memory problems, and poor thinking abilities (dubbed “depressive pseudodementia”). So, if someone goes from depressed to non-depressed, and stays non-depressed for quite some time, should cognition not improve? In other words, if ketamine effectively treated their depression (which it reportedly did), should there not be an increase in cognition between baseline and timepoint X? Did neurocognitive domains indeed improve but the improvement was then masked (or erased) by gradual neurotoxicity?
In sum, we can say that ketamine used at “party doses” is almost certainly neurotoxic but the jury is still out on whether ketamine at therapeutic doses is or not.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Mechanism of neurotoxicity
There are multiple potential mechanisms. The most likely mechanism is the following. NMDA receptor blockade leads to an increase in extracellular glutamate, which then activates AMPA receptors in excessive amounts. The excessive AMPA receptor activation then leads to a sharp influx of calcium, which then kills neurons by excessive excitation (excitotoxicity) through both apoptosis and necrosis. This excitotoxicity most likely happens during the ketamine high.
Supplements such as N-acetyl-cysteine may help to counteract it to a small degree. Coadministration of benzodiazepines can prevent some of the excitotoxicity – but unfortunately also part of the therapeutic effects.
Psychedelics and ketamine trigger some of the same intracellular signaling pathways (e.g., BDNF -> TrkB -> mTOR). Like ketamine, psychedelics trigger an increase in neuroplasticity (spinogenesis and synaptogenesis) but they are not known to be neurotoxic. Unfortunately, psychedelics can occasionally cause HPPD, which can, in severe cases, be incredibly distressing.
But isn’t ketamine neurogenetic?!
What most people mean when they say something increases neurogenesis, they mostly mean it increases neuroplasticity, which, for practical purposes is limited to the generation of dendritic spines (spinogenesis) and synapses (synaptogenesis). Spinogenesis and synaptogenesis are very different from neurogenesis (the birth of new neurons). Neurogenesis is limited to two sites in the human brain (the hippocampus and the subventricular zone) and a local creation of neurons in these sites cannot make up for the death of functionally integrated neurons elsewhere. So, ketamine increases neurogenesis in two small brain sites (like most other antidepressants) and it also increases neuroplasticity (at least for a couple of days).
Local neurogenesis plus synaptogenesis & spinogenesis are reversible and usually short-lived (weeks) but dead neurons will never undie.
Given that Spravato (esketamine nasal spray) has been widely available and so-called “ketamine-clinics” proliferated, we are possibly going to have an answer to the question regarding whether and the extent of ketamine neurotoxicity soon. In the meantime, it is probably prudent to err on the side of caution.
My gut feeling is that people who are doing ketamine at even therapeutic doses regularly are more likely than not to give themselves non-negligible amounts of irreversible brain damage.
Unfortunately, ketamine has become a frequent drug of abuse at doses far higher than therapeutic doses. Similar to MDMA (although by a completely different mechanism), the neurotoxicity caused by high doses is irreversible. It is also quite worrying to see ketamine clinics mushrooming everywhere, with some patients reportedly going in twice per week and being given infusions of 100mg or more, which, considering the doubled bioavailability compared to inflation, is definitely in the “party dose” territory. As so often, hype and industry are about to destroy something that was originally quite useful in select cases.
Related articles on drugs of abuse
- Thoughts on THC
- Thoughts on Opioids
- Ketamine is Probably More Neurotoxic Than You Think
- Why Does Nobody Talk About Hallucinogen Persistent Perceptive Disorder?
- How Neurotoxic is MDMA?
- Is Adderall/Vyvanse Neurotoxic?
Sources & further info
- Scientific article: Ketamine: Neuroprotective or Neurotoxic?
- Scientific study: Brain damages in ketamine addicts as revealed by magnetic resonance imaging
- Scientific study: A review of potential neuropathological changes associated with ketamine
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.