
Naltrexone is a potent opioid receptor antagonist. In the clinical setting, naltrexone is sometimes prescribed for opioid or alcohol dependence, specifically to block the feeling of “pleasure” and to reduce “cravings”.
However, given at extremely low doses, about 1/50th to 1/10th of clinical doses, low-dose naltrexone (LDN) has a couple of interesting properties. LDN seems to modulate a variety of systems, including the reward system, hypothalamic subsystems, and the immune system.
Potential benefits range from helping with all kinds of addictions (including behavioral addictions), low libido, fibromyalgia and other pain states, chronic fatigue syndrome, long COVID, burnout, and low-level inflammation. However, it remains to be seen whether LDN is more hope than hype.
Personal experience
After reading about LDN and its many potential benefits, I decided to try it out myself. I mostly did this out of curiosity. Secondary goals were potentially greater energy levels (as naltrexone is known to disinhibit POMC neurons), reducing cravings (I was craving a lot of chocolate at the time), and a higher hedonic tone (enhancing the depth of my emotions).
Naltrexone is a mu-receptor antagonist – meaning it blocks the receptor that heroin, oxycodone, and fentanyl act on. It is therefore an “anti-pleasure” drug.
Fortunately, pharmacies in my country carry a liquid version of it, which is easy to microdose. I took my first dose (0.5mg) in the early evening. I got a little tired but did not think much of it. That night, my Oura ring showed a 60% reduction in slow-wave sleep and a 100% increase in REM sleep. My dreams were very vivid.

The next day, I took 1mg in the morning. 2-3h after dosing, I got very tired and I could barely keep my eyes open at 9 am. To counter the tiredness, I made some black tea (I usually do not consume caffeine and caffeine is my “secret weapon”). This did nothing.
Because I had to work on a paper, I added a low dose of modafinil sublingually, which is usually very strong for me. However, this did not help much either. Playing 4D chess with my biology, I added 200mg of dexibuprofen, which sometimes works wonders in times of unexplainable fatigue. Nothing. Strange.
At around noon, I started to feel “weird”. Everything felt “colorless” (hard to describe). I went for a walk and listened to some music. I felt nothing. Later that day I had a conversation with a friend about topics that usually captivate me. Again, nothing.
Towards the evening, I wanted to go to bed early (and I should have). However, a girl I was dating at the time and had a strong crush on said that she would come over to my place. As she was sitting in front of me, I could not feel any sparkle, which I think she noticed. Then, as we were making out, I again felt nothing.
This has given me a taste of what true anhedonia feels like. Anhedonia is discussed here.
If such a state would go on for much longer, I can totally see how people turn to hard drugs or other extreme behaviors just to feel something. Perhaps even, some people others look up to (e.g., actors, musicians), feel like this all the time – all empty inside. Anyway, this experiment has shown me that my mind is all I have and if my mind is screwed, my life is screwed.

Even though LDN is supposed to be taken for a couple of weeks before significant benefits can be noticed, I immediately stopped it. After two trance-like days during which I could feel neither positive nor negative emotions, I was back to normal. I now know that, for me, the other side of the opioid system is off-limits as well.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
A good friend of mine had a similar experience. On day two of taking LDN he went on a skiing trip with his dad. Despite the beautiful scenery and company, he said that everything was just dull and grey. In the mindset he was in, he could not understand why people get up from their beds in the morning to do this – although he usually loves skiing.
Another friend, who takes LDN to help with long COVID, also reported feeling quite anhedonic and lifeless after every dosage increase. Another friend, who is a good candidate for LDN because of suspected low-level inflammation, did not feel much other than some dizziness. And a former client of mine with erectile dysfunction issues had a good response to LDN, which he tried after extensive hormone optimization and a handful of other pharmaceutical options failed.
It is interesting how people sometimes react very differently to the same neuropharmaceutical drug, likely reflecting their individual genetic, neurobiochemical, hormonal, and brain-structural differences. In sum, as with most other neuropharmaceuticals, the best way to figure out whether it works or not is simply good old trial & error, and patience.
How it works
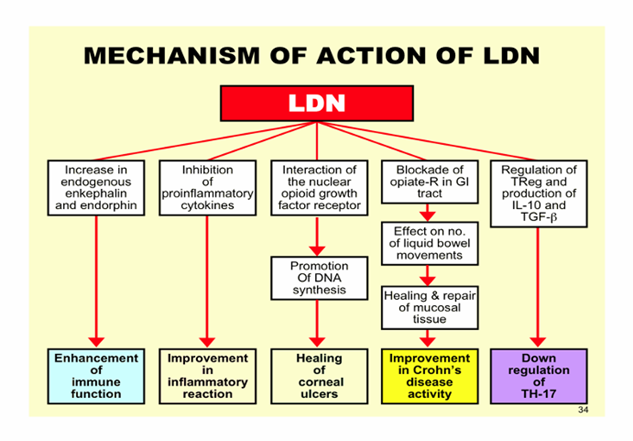
Naltrexone is an antagonist at the mu and kappa-opioid receptors – the opioid system is discussed here. Among many other functions, mu-inhibitors block euphoria and kappa-inhibitors can banish dysphoria. Next to their involvement in the hedonic system, these two receptors are distributed widely throughout the brain and are involved in a variety of other functions.
Therefore, LDN’s “exact” mechanism of action remains elusive, and possibly also varies depending on the disorder one tries to treat. I will now discuss what I believe to be the two categories in which LDN may be most useful.
- Addiction: Given the way it interferes with the endogenous reward system, it is reasonable to assume that LDN is a potent add-on treatment for all kinds of addictions, including behavioral addictions such as binge eating or pathological gambling. Even though it is currently only used officially for treating alcoholism, opioid addiction, and food addiction (as part of the drug Contrave), its “anti-craving” benefits presumably extend to many other addictions as well.
- Chronic inflammation or immune dysregulation: Also lymphocytes carry mu-opioid receptors. Given that naltrexone modulates immune cells as well as acts on a variety of hypothalamic control centers, it may help with states of immune dysregulation, such as chronic pain states, fibromyalgia, or ME/CFS.
The connection between inflammation, depression, anhedonia, and lethargy is discussed in more detail in my article on ibuprofen.
Other experience reports
For a discussion of the molecular correlates of well-being, and links to accounts of various related molecules I have experimented with, read here.
For a full list of experience reports click here.
Sources & further information
- Anecdotes: Reddit – r/LowDoseNaltrexone
- Scientific review: Low-Dose Naltrexone (LDN)—Review of Therapeutic Utilization
- Website: Wikipedia – Low-dose naltrexone
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.