
What follows is a list of potentially interesting neuropharmaceuticals that are either stuck in pharmaceutical pipelines or were withdrawn from the market. Here and there I´ll add in a couple of general comments about neuropharmacology.
After writing this article, I was tempted to try two of them, pitolisant and NSI-189.
NSI-189
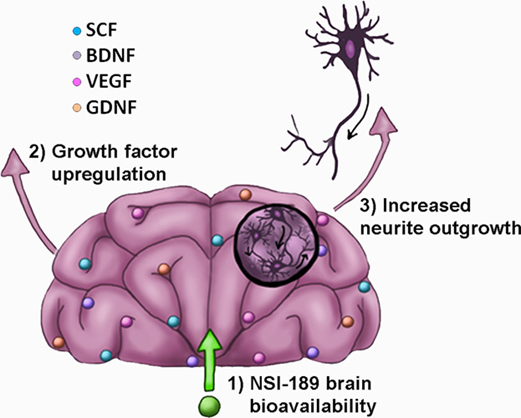
NSI-189 is a still experimental compound that is being developed for major depression and a variety of forms of cognitive impairment. It is thought (and hyped or hoped) that its effects hinge on stimulating neurogenesis.
Because there was some interesting and convincing data on the molecule (including safety data), I decided to guinea-pig with it. My experience with pitolisant here.
Nomifensine
Nomifensine is a dopamine-noradrenaline reuptake inhibitor (NDRI). On paper, nomifensine is quite balanced with respect to its NRI and DRI effects. It was used extensively in the 1970s and 1980s for unmotivated and melancholically depressed folks. It is probably a little more intense/effective than bupropion for its increased DAT-receptor affinity. However, it was withdrawn from the market because of a rare (but life-threatening) hematologic side effect.
Amineptine
Amineptine is structurally related to tianeptine. Both were created by the same French manufacturer (Servier). Furthermore, both are structurally classified as “tricyclics” though they are fundamentally different from other tricyclics. While tianeptine is a weak mu receptor agonist, amineptine is a relatively selective dopamine reuptake inhibitor (and weak releaser), though it does also weakly inhibit the reuptake of noradrenaline.
Based on its pharmacological profile (and anecdotal reports) it could be regarded as “modafinil with a punch”. Reportedly, it is much more stimulating than modafinil and causes a subtle euphoria. Furthermore, it is known to have strong pro-sexual effects, and, anecdotally, it can cause spontaneous orgasms for some people. It was also used as a doping agent similar to amphetamine.
The half-life of amineptine and its metabolites is only about 1-3 hours, and therefore it does not disturb sleep (unlike modafinil).
Uniquely among dopaminergic compounds, amineptine was predominantly used as an antidepressant. It was withdrawn from the market in the year 2000 due to concerns about its abuse potential and liver toxicity (though very rare). Unfortunately, amineptine production was stopped in 2005 and it does not seem to be available anymore in any country worldwide – at least officially.
Weirdly, the FDA recently placed amineptine in Schedule I even though pretty much nobody abuses it (given that it ceased to be made a long time ago). The philosopher David Pearce has supposedly been taking it daily since 2001 and had his own stash custom-synthesized in China.
It is unlikely that we will ever again have antidepressants like amineptine again. Before making it to clinical trials, all molecules are screened for whether they cause self-administration in lab rats (as a proxy for addiction potential). If they do, which applies to the vast majority of dopaminergic drugs, they are usually thrown out long before they are ever tested in humans. According to David Pearce, “probably not the best strategy for finding life-enriching molecules”.
Pitolisant
Pitolisant (Wakix) is the only molecule on this list that is currently an approved drug, though tesofensine and ansofaxine could soon follow. Pitolisant is an H3 receptor antagonist, which is an inhibitory autoreceptor on histaminergic neurons. As such, pitolisant dis-inhibits histamine release in the CNS. In theory, this causes wakefulness without dopaminergic or adrenergic stimulation. The neglected importance of the histamine system is briefly discussed here.
Because I found the molecule very interesting on paper (and because the drug is readily accessible to me because I am an MD), I decided to experiment with it. I discuss my experience with pitolisant in more detail here.
Pitolisant
Pitolisant (Wakix) is the only molecule on this list that is currently an approved drug, though tesofensine and ansofaxine could soon follow. Pitolisant is an H3 receptor antagonist, which is an inhibitory autoreceptor on histaminergic neurons. As such, pitolisant dis-inhibits histamine release in the CNS. In theory, this causes wakefulness without dopaminergic or adrenergic stimulation. The neglected importance of the histamine system is briefly discussed here.
Because I found the molecule very interesting on paper (and because the drug is readily accessible to me because I am an MD), I decided to experiment with it. I discuss my experience with pitolisant in more detail here.
Diclofensine
Diclofensine is a triple reuptake inhibitor (inhibiting the transporter of all three major monoamines) whose development was abandoned due to unknown reasons. It potently inhibits the reuptake of dopamine and noradrenaline but it also inhibits the reuptake of serotonin to some extent – a DAT:NET:SERT ratio of about 1:1:3.
However, it should be mentioned that a drug with the same molecular binding profile (i.e., the same ratio of molecular targets) might be quite different in its effect from another drug with the same binding profile because it is also important to consider how the drug interacts with its targets.
What is the exact target site? What does molecular binding do to the structure and function of the target protein? Does the drug bind and remain stuck or does it have a specific on-off rate? These and many more factors ultimately determine how a drug “feels”.
Tesofensine
Tesofensine is another triple reuptake inhibitor, which may soon be available for clinical use. As a cocaine analog (i.e., they considered the molecular structure of cocaine and tweaked it to make it a little less powerful and longer-acting), it is a triple reuptake inhibitor with a NET:DAT:SERT ratio of about 1:2:3. It only needs to be given at very low dosages (about 1mg/d) and has a half-life of 9 days. It is currently in Phase III for the treatment of obesity but it may potentially prove useful for a host of other psychiatric disorders as well.
In fact, triple-reuptake inhibitors such as tesofensine or ansofaxine (discussed shortly) are thought to be useful for a wide range of disorders: depression, anxiety, addiction, ADHD, obesity, and dementia.
The “one pill regimen” is convenient and increases patient compliance (as most people would rather take one pill than two). However, if pill-taking is not an issue, in theory as well as in practice, triple reuptake inhibition could also be achieved by “creative neuropharmacology”, for example, the combination of escitalopram + reboxetine + modafinil.
The advantage of the “customized” approach is the possibility for individualized “finetuning” with respect to the different monoamines. However, even if the binding profiles are similar, the effect may still be quite different, depending on how the molecule binds to the target (as discussed earlier).
As always, optimal dosage and drug regimen are best discovered by cautious empirical self-investigation.
Bromantane
Bromantane is a cousin of memantine, an NMDA-R antagonist used for dementia, and amantadine, a drug used in the treatment of the flu. It is officially used mostly in Russia.
Its exact mechanism of action is not understood but it (reportedly) seems to increase dopamine signaling without any effect on the dopamine transporter. In my opinion, the widely broscience-perpetuated “fact” that bromantane is a “dopamine synthesis enhancer” is probably untrue.
Interestingly, amantadine, a chemical cousin of bromantane, is an agonist at the sigma receptor, whose ligands may have potential therapeutic uses for a variety of conditions, including depression, addiction, and neurodegenerative diseases.
The sigma receptor is unique in that it does not fit into any of the traditional categories of receptor proteins. It shares some structural features with G protein-coupled receptors (GPCRs) and ion channels, but also exhibits properties that are distinct from both.
Nonetheless, even if bromantane turns out to be a sigma receptor ligand, I do not know what to make of that.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Apimostinel
Apimostinel is a weak positive allosteric modulator of the NMDA receptor. Like ketamine, its effects are (reportedly) rapid and long-lasting. A few years ago, a forerunner of this drug (rapastinel) was on Breakthrough Therapy Status for treatment-resistant depression, however, it failed development. Apimostinel is a modified version of rapastinel that is more potent and orally active. It is currently in Phase I and Phase II for the treatment of MDD.
CX171
CX171 is an AMPAkine, a drug that modulates the AMPA receptor in a similar way benzodiazepines modulate the GABA-A receptor.
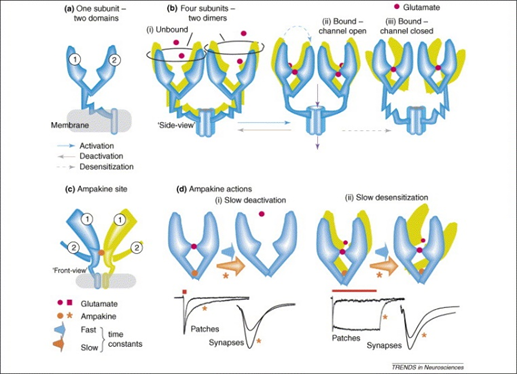
Improved glutamate signaling may help with cognitive impairment, ADHD, MDD, and the negative symptoms of schizophrenia. Unfortunately, elevating glutamate levels too much is neurotoxic. Currently, there are no approved drugs that amplify glutamate signaling other than piracetam and ketamine.
Mazindol
Mazindol is a sympathomimetic amine, similar to ephedrine or amphetamine. In the 1960s it was used as an anti-obesity drug. Currently, it is being investigated for ADHD. With a daily dosage of only a few milligrams and a half-life of around 10h, it seems to be quite useful. It is still sometimes used off-label for weight loss purposes, though stimulants, in general, are gradually being replaced by GLP-1 agonists such as semaglutide.

Naphthylaminopropane
Naphthyl-amino-propane is a slight releaser of serotonin, dopamine, and noradrenaline in a ratio of 1:4:4. It is supposedly a little less stimulating and a little more “chill” than amphetamine, possibly due to having a stronger effect on the serotonin levels (amphetamine has only a weak effect on serotonin).
The drug is currently being investigated for its usefulness against stimulant addiction (or better: swapping out one addiction for another). Because it is also an agonist at the 5HT2C receptor, it has appetite-suppressing properties, for which it was initially investigated.
It is chemically related to sibutramine. Sibutramine was used as an appetite suppressant that was withdrawn from the market because of an increased incidence of cardiovascular events such as heart attack and stroke.
Tametraline
Tametraline is structurally related to sertraline (Zoloft). Instead of acting on the SERT + DAT (like sertraline), it inhibits NET + DAT. However, Pfizer discontinued its development. Based on its binding profile, it may have been a useful alternative to bupropion. However, as mentioned earlier, it is quite hard to bring new stimulant-like antidepressants to market because of their addiction potential.
Dasotraline
Dasotraline is another metabolite of sertraline. However, in contrast to sertraline (SDRI) or tametraline (NDRI), dasotraline is a triple reuptake inhibitor. It is currently being investigated for its use in MDD, ADHD, and binge eating disorder. A similar drug, indatraline (also a sertraline derivative), is currently being investigated for the treatment of cocaine addiction.
Amitifadine
Amitifadine is a triple-reuptake inhibitor with a SERT:NET:DAT ratio of 1:2:8. It was under development for depression but failed Phase III in 2013. Currently, it is being investigated for smoking cessation, alcoholism, and food addiction.
As might be evident by now, different pharmaceutical firms are trying hard to bring triple reuptake inhibitors to market. Most of these drugs would have probably succeeded 20 years ago, but nowadays the FDA and EMA are more strict and getting drugs approved has gotten a lot more difficult.
Ansofaxine
Ansofaxine is currently being investigated in multiple countries for major depression and is in Phase III in the US and China.
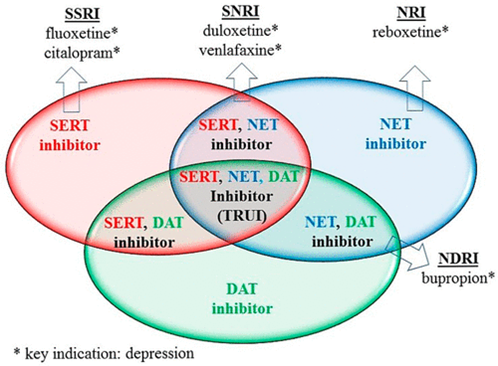
It is structurally related to venlafaxine (Effexor – marketed as “Prozac with a punch”). Venlafaxine has a SERT:NET ratio of 15:1. So, contrary to popular belief, it is not really an SNRI but rather an atypical SSRI (SSRIs are discussed here). In contrast to venlafaxine, ansofaxine seems to be pretty balanced between all three monoamines, with a slightly stronger action on dopamine.
Most antidepressant treatments do not directly enhance DA neurotransmission, which may contribute to residual symptoms, including impaired motivation, concentration, and pleasure. So, should this drug gain approval, it might become a new blockbuster drug – and psychiatry may finally start to appreciate the crucial role of dopamine for mood, life enjoyment, drive, self-confidence, and emotionality. The brutal neglect of dopamine is discussed here.
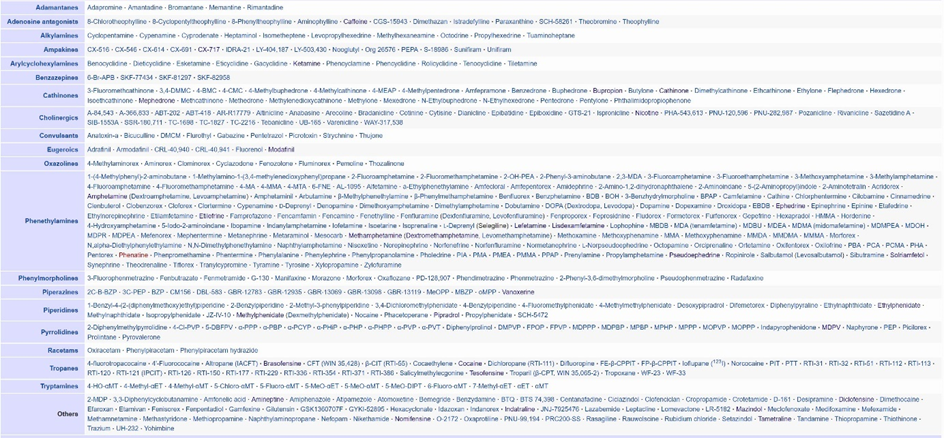
Others
Below is a screenshot of the many known stimulants, many of which are quite unexplored by the recreational, nootropic, broscience, and scientific communities alike. A like to the image below here.
Sources & further information
- Website: Table of stimulants shown above
- Website: Wikipedia – Triple-reuptake inhibitors
- Anecdotes: Reddit – r/ObscureDrugs
Disclaimer
The content on this website represents the opinion and personal experience of the author and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without a doctor’s supervision. The content presented is exclusively for informational and entertainment purposes. Never disregard professional medical advice or delay in seeking it because of something you have read on the internet.