
Disclaimer: I have never personally met Bryan Johnson. Reading this again, I realized that this article is quite harsh at times. Overall, I do like him and I am grateful that someone like Bryan exists as he is propelling the whole field of longevity forward by making it more popular. I also like the way he deals with criticism. While reading this article, please keep in mind that this is an opinion piece, and some of the points I make are hypothetical.
In my early twenties, I had a multi-year-long period during which my body fat was ultra-low (4.8% on the only DEXA scan I had done during that time). I became very obsessive and tolerated an unbelievable amount of self-torture to reach my goals. I also developed very weird eating habits and was rigid about my meal timing – I could not stand breaking my fasts by even a few minutes.
My need for control was extreme and I meticulously tried to control my environment. In retrospect, I am sure that keeping my body fat that low was actually the single biggest contributor to my 90-degree personality turn (as compared to my adolescence) – in other words, I behaved the way I did because of my eating disorder and not the other way around.
During this time, my blood pressure (roughly 105mmHg), resting heart rate (low 40s when sleeping), and body temperature (roughly 35.8-36.5) were all very low. I had a fixed caloric intake (2000-2100kcal/day) and whenever I overshot it I made sure to balance it out over the next couple of days. My face looked pale and gaunt. My vitality was non-existent.
Just like Bryan, I was never underweight because I had a fair amount of muscle. I had an eating disorder concealed under the veil of “health and fitness”. However, what was really going on was starvation. Nowadays, I quickly recognize it when someone else has an eating disorder.
When body fat gets to very low levels, for evolutionary reasons, people are set to become obsessive, rigid, and engage in OCD-like behaviors intended to help with foraging. We see this in about every mammal we study, and Bryan Johnson is no exception.

Upon starvation, sympathetic nervous system activity falls, leading to low blood pressure (as far as I know, Bryan’s is around 105mmHg systolic), heart rate, (Bryan’s is in the low 40s while sleeping), and body temperature. Sympathetic activity is the biggest contributor to the basal metabolic rate (how many calories you burn while doing nothing). Whenever we eat less than we expend, the nervous system decreases sympathetic activity. In starvation states, the nervous system shuts it down to very low levels in a desperate attempt to conserve energy.
In anorexia nervosa (including atypical anorexia nervosa – the same state without being underweight), body temperature often falls to 36C – 35.5C, so borderline hypothermia. This lowering of the hypothalamic temperature setpoint is also a frantic last-ditch effort to have the body expend less energy.
Bryan just released a newsletter this week “bragging” that his body temperature hovers around 34.8C, which means outright hypothermia. For the last couple of months, I worked in emergency medicine and whenever someone had outright (acute) hypothermia we would put the patient into the observatory critical care unit. Mammalian enzymes have evolved to function well within a very narrow temperature range and when the temperature is considerably above or below, kinetic equilibria are going to be perturbed.
To quote from his newsletter: “My health program has me metabolically cold plunging. Since starting Blueprint, my body temp has cooled 4°F in 3 yrs, now at 94.8°F. This technically qualifies as minor hypothermia. To put this into context, it takes swimming more than a mile in ice to achieve an equivalent temperature reduction as mine.”
Well done, Bryan.
While, in theory, having a colder body temperature may be related to longevity (simply put, the lower the temperature the slower chemical reactions happen), in the “wild” this may be a double-edged sword because at lower temperatures the immune system is less capable (predisposing to infections & cancer) and also repair processes happen more slowly. Most importantly, at these temperatures brain function is quite impaired because of the perturbation of the delicate balance of ion kinetics.
In other words, an average animal with hypothermia in the wild is usually dead long before its maximum lifespan kills it. However, Bryan is not like an animal in the “wild” but rather living in his own “lab”.
Further hints of him being in a state of starvation are his carotenemia, which nearly every anorexia patient has, and his remarkable pallor – most people think that he is so pale because he simply avoids the sun. Actually, his body is so cold and his blood circulation is so centralized that there is little cutaneous blood flow, therefore the red color of hemoglobin does not “shine” through the skin causing his vampire-like color.
Also, in the interviews I have seen of him, his blinking frequency is quite high. Keratoconjunctivitis sicca (dry eyes) is relatively common in restrictive eating disorders (or at least often exacerbated by it).
Bryan’s (excessive?) exercise regimen in combination with his nutritional state may be causally related to the impairments of his heart and musculoskeletal system (some data and more on that later). Hyperactivity and “excessive drive for exercise” are hallmark signs of the most common type of anorexia. Relatedly and paradoxically, if we experimentally starve mice, instead of “saving energy by doing nothing” they run or work themselves to death. The restlessness associated with starvation is presumably an evolutionary adaptation to help with foraging for food and may be caused by the low leptin levels associated with very low levels of body fat.
In sum, it is not too far-fetched to assume that as Bryan started to control “Evening-Bryan”, he gradually fell into an eating disorder. The resulting neurobiochemical makeup may be causally intertwined with the evolution of many of his current ritualistic behaviors.
I discuss the neurobiological basis for this in more detail here: The Syndrome of the Ultra-fit
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
What are my overall thoughts on Bryan?
As explained in my article on diet, the “optimal” nutrition is individual (e.g., genetics, age) and context-dependent (e.g., activity levels). Furthermore, there is quite some variability and many people can function quite well on a variety of different diets. Moreover, vitality and longevity can probably not be maximized at the same time. So, when someone claims to have found the “perfect” nutrition, the person is either scamming or not understanding much.
The part I disagree with most is his self-starvation (Disclaimer: I am biased due to my personal experience). I would like for Bryan to communicate openly how much “like shit” he feels all the time (fatigued; weak; cold; hungry; etc.). This is not due to his program but primarily due to his insufficient caloric intake, and more importantly, combined with having ultra-low body-fat levels seemingly year-round. From a longevity & health perspective, he would do well with leptin injections (or simply gaining a little body fat). However, they would change his neurobiochemistry probably in a way that is not conducive to maintaining his rigid lifestyle.
While caloric restriction may be helpful for longevity, it means sacrificing most of his (biological) vitality. Furthermore, this is a big MAY in already long-lived mammals such as great apes, elephants, and dolphins – particularly if they live in the wild as caloric restriction leads to immunosuppression, poor wound healing, and a host of other adverse effects.
Someone with a blood pressure and body temperature this low is definitely not “healthier than most 18-year-olds”. The metrics he is using to judge that are quite theoretical but more on some of his real data later.
Furthermore, he claims that he is “aging more slowly than 88% of 18-year-olds”. He uses a number of epigenetic clocks (e.g., PCHorvath 1, PC Phenoage, etc.) to determine his speed of aging. Evidence suggests that they advance faster during periods of rapid growth and development. Given that puberty is probably the time period with the fastest rate of aging in life, beating 18-year-olds is not an accomplishment. Furthermore, most of the epigenetic clocks are quite faulty. For example, when someone fasts for a couple of days, these clocks tend to age-reverse by a couple of years (for a short time only). Bryan’s “starvation mode” may be keeping these clocks down artificially and if he were to spend a couple of months on a normal diet, this may drive these clocks back up by a decade or more.
I do not believe in the validity of his sleep data. In starvation, sympathetic nervous system activity and noradrenaline levels get very low, which causes sleep resting heart rate to drop and heart rate variability to increase. While having a low RHR and high HRV can be suggestive of restorative sleep (e.g., as they do with increased cardiovascular fitness or with low cortisol levels), the change in these parameters can also be suggestive of an abysmally low sympathetic activity. Hence, one could argue that Bryan “cheats” his way to a great sleep score by having a pathologically low sympathetic tone, which the sleep trackers presumably mistake for being in a state of deep relaxation and having a very restorative sleep. Moreover, different sleep trackers give you different results, sometimes vastly so. Is he just wearing the one that gives him the best results? What happens if he switches from Whoop to e.g., Oura ring?
I also think he is sometimes dishonest about where his on-paper results are coming from. He takes potent anti-aging drugs (rapamycin, metformin, acarbose, 17-alpha estradiol), uses a bunch of hormones (thyroid hormones way higher than replacement doses; 17-alpha-estradiol, TRT in the past; growth hormone in the past), and even gene therapies. His nutty pudding has little to do with his results, yet this is what is being fed (and sold) to the masses.
While the testosterone dosage was still listed on his website, the way he looked while taking “TRT” looked nothing like a “testosterone replacement dose” but rather like a (mild?) steroid cycle, particularly at his low caloric intake. Remember, the man is 45 and not 18. In his defense, he does look much bigger than he actually is because his body fat is very low, enhancing muscle definition so him being 100% transparent here is still in the cards.

Yet, given that veins vasoconstrict in non-hot water (particularly in somebody with poor cutaneous blood flow), I would guess that he somehow artificially enhanced vasodilation before the photo shoot, either by taking a vasodilator (e.g., Viagra), using a blowdryer or sauna, and/or getting in a pump through volume training.
It seems that he is spending a lot of his time & effort on maintaining his hair (huge kudos for admitting that!). He should not need to do that if his body was functioning like an 18-year-old. It is true that androgenic alopecia is mostly a time-course disease due to a genetic susceptibility to DHT (among other things) but Bryan is using topical 5-alpha-reductase inhibitors, and if Bryan truly set back his true aging clock he probably would not be battling with ongoing hair loss (despite a plethora of interventions), or at least it would mostly halt – which does not seem to be the case.
And through his implementation of vast amounts of cosmetic interventions he is concealing his true speed of aging in the same way he is concealing his true pallor through the skilled use of make-up. However, I love the fact that he shares these as normally people do these in private and like to credit their “good genes” for their looks.
I do think that what he does is interesting. I read his protocol and watched a few of his videos. The only thing I adopted myself was taking 1mg of lithium per day. I would be interested in measuring my nighttime erections and seeing how they change as my sex hormones, calories, body fat, stress levels, leptin levels, etc change.
The part about Botox injections into his penis was superb and ever since seeing that my opinion of him was swayed from rather negative to rather positive – particularly because he is being public about this. I do think that this single tweet might have opened up a new industry…
Even though this article is full of criticism, more and more I find myself liking him than not liking him. I particularly like him calling out AG1 and other shitty companies. I also like his “shot-gun” approach: “Let us try everything at once and see what we find.”
I am also impressed by how well and courageous Bryan reacts to the vast amounts of hate and criticism he gets. We are social primates and social humiliation and ostracism trigger deep-seated circuits of fight or flight – Bryan does neither and it does take a certain greatness to react the way he does (though I am sure he has PR consultants).
Much of his undertaking is probably for his own ego, which seems to be hungry for attention (I could be wrong!). He says that his main goal is all about “not dying” and surviving until superintelligence hits. To me, this seems questionable. Firstly, he is around 45 years old and most predictions about the advent of AGI are way shorter than 40-50 years. Why then take these risks by plunging into the unknown?
Secondly, it seems that quite a few people hate him, perhaps unjustified but still. Given that the US society has many lunatics, by being so public-facing he exposes himself as a target of hate crime, meaning that he incurs the additional risk of homicide, which may even be his biggest risk of death. He has roughly half a billion $, if not more. If “Don’t die!” is really his top and only priority, why not just take your money & your interventions and spend the rest of your time within a very sheltered property in New Zealand without telling anyone?
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Some more data
Sure, he is in the “top 1%” in some parameters (e.g., fat mass, inflammation, VO2 max, bone mass – for which he may have used teriparatide) but he is much worse off in a number of other parameters that cannot be improved via “effort” (e.g., physical training, medications). Below is cherry-picked data taken from his Blueprint website revealing some of his weaknesses, which he rarely discusses as far as I am aware. Disclaimer: I picked the most negative data I could find and there is definitively a wealth of positive data!
- He has 1.37 liters of subcutaneous fat. This is incredibly low and approaches body-builder-level territory. He calls this “optimal”. Subcutaneous fat is healthy – it is the visceral fat that is bad.
- Some of his heart parameters are like that of a 70-year-old (“LV septal A’ mitral: age 70+; Aortic root diameter age 70+; LA E’ laterobasal: age 70+; RVSP: age 70; LV sepal E/E’: age 55). Despite being a doctor, I had to look up some of them myself. I will briefly explain what these mean.
- “LV septal A mitral” (age 70+) is a marker of diastolic function in the left ventricle. His value of age 70+ means that there is stiffness in the heart muscle, meaning that the heart can not relax as well during diastole, often associated with older age.
- Aortic root diameter (age 70+): This is the diameter of the lowest part of the aorta. The diameter increases with age due to normal “wear and tear” (e.g., hypertension, overexercising). A large aortic root diameter predisposes to aortic dissection, which is very rare, but usually deadly when it occurs.
- “LA E’ laterobasal” (age 70+) is very similar to the first value. This measures the relaxation velocity of the lateral basal wall of the left atrium during early diastole (vs. the first value measures something similar but for the left ventricle instead of the atrium). It seems that the left side of his heart is not the best at relaxing (i.e., becoming soft while being filled with blood).
- “RVSP” (age 70+) stands for right ventricular systolic pressure, which is an estimate of the pressure in the pulmonary artery, which is mildly elevated. My non-cardiologist understanding of the heart tells me that this could be related to the diastolic weakness of the left side of his heart. Pulmonary hypertension is a serious matter. Bryan has not commented on his pulmonary pressures as far as I am aware.
- “LV sepal E/E’” (age 55): He scored age 55 meaning that his heart is about a decade stiffer than what we would expect for his age.
- Note: It is possible that his bad heart markers are due to a combination of overexercising + undereating. If this is indeed the case, then they will continue to get worse over the next couple of years unless Bryan changes key aspects of his protocol. Of note, structural changes to the heart are commonly observed in long-standing anorexia nervosa. It is also possible that his values are the way they are mostly due to genetic predisposition and his program has little to do with it. To say for sure, we would need data on how these values changed since Bryan started Blueprint.
- Most of his brain markers are around his biological age (“White Matter Hyperintensities: age 48; Ventricular volume: age 48; Cortical grey vol: age 45; AI T1 brain age: age 44; RAVENS PM: age 41, Total Cerebral WMV: age 37; WASO: age 37). The prolonged starvation and the associated hormonal decline may be responsible for the white matter hyperintensities in his brain (early onset grey matter atrophy), and not just his internal jugular vein stenosis as he believes. Cortical atrophy has been reported in primate studies looking at the effects of starvation on longevity.
- His joints and tendons do not seem to be in the best shape, particularly the important joints of the knee and shoulder. Next to the heart, these impairments of some parts of the musculoskeletal apparatus are probably among his weakest areas. I suspect that some of these are the result of under-eating + over-exercising + under-resting:
- “Bilateral shoulder labral degenerative tears with paralabral cysts.” They are unlikely to get better other than with labrum surgery.
- “Tendinosis on both sites of the supraspinatus rotator cuff (shoulder) with subacromial bursitis (chronic inflammation in R>L shoulders).” Chronic degeneration of some shoulder tendons. May improve with time.
- “Bilateral knee chondromalacia patella with left knee mild to moderate effusion/bursitis.” Cartilage wear beneath the kneecap to the point that there is inflammatory fluids in his knees. This is unlikely to get better because cartilage barely heals – at least with conventional treatment. I would be interested to know whether the stem cell treatments he did made any difference.
- “Bilateral hip gluteus medius tendinosis.” Chronic degeneration of the tendon of the glute medius – probably due to overtraining. The glute medius is a very important and neglected muscle and I am sure Bryan is aware of that – perhaps a little too much.
- “Bilateral Hip Cam impingement syndrome.” Can predispose to osteoarthritis of the hips.
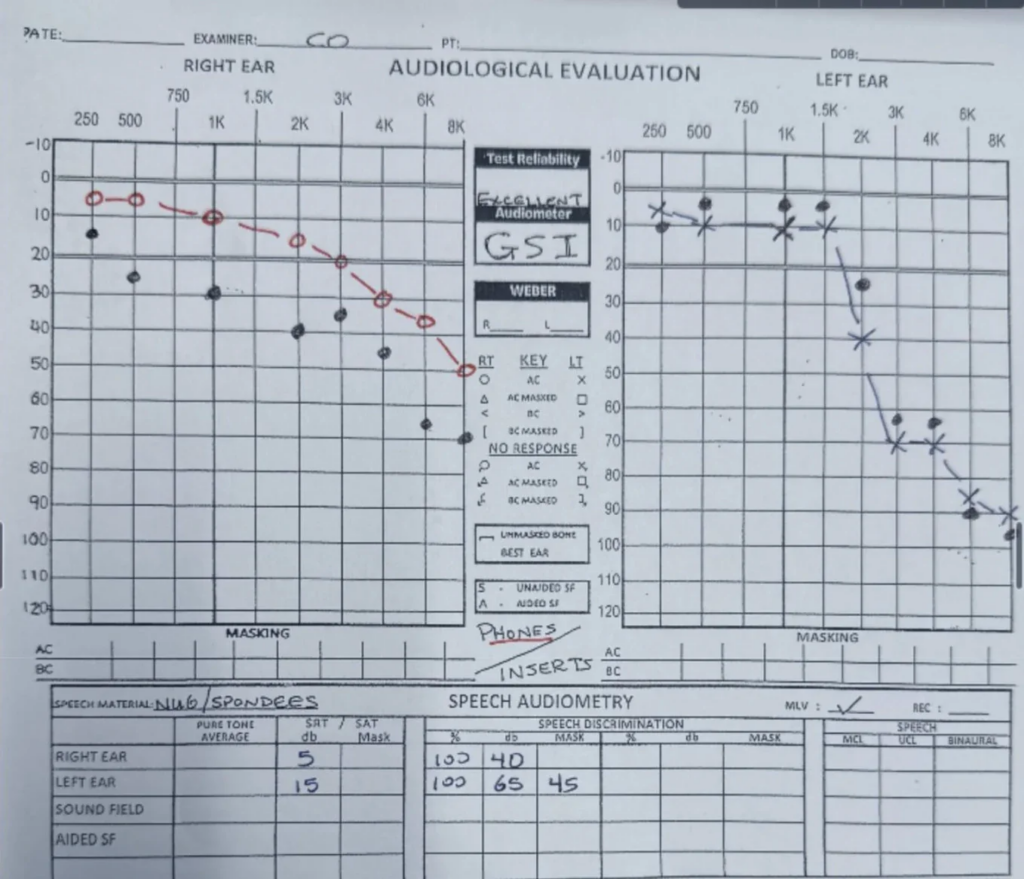
- His hearing is not the best (Right ear normal freq: age 61; Left ear normal freq: age 51; Right ear EHF: age 60; Left ear EHF: age 32). PDE5 inhibitors are known to damage hearing. Actually, reading his data again, his hearing is quite shitty and seems to get worse over time. At age 45, he is significantly hearing-impaired in both ears. Bryan Johnson does take tadalafil, which is known to damage hearing. I suspect that this may even be his main reason why his hearing is getting worse over time despite the “I do not expose myself to loud noise” neurosis he has. Below is his audiogram – terrible. The black dots in his right ear suggest that he is getting worse over time. A healthy hearing has dots between 0 and 10 at least up until 4k Hz. He is worse than that at pretty much every point.
- His telomere length is that of a 42-year old so roughly what we would expect.
- In 2021 he writes: “Body fat increased from 3.5% to 6% due to transitioning to three meals a day (10-16 hour fast), from one meal a day (~22 hr fast).” Most people cannot even imagine what it feels like to be 3.5% body fat, which is in life-threatening territory by the way.
Somewhere buried on his website he writes: “Severe headache symptoms causing to wake in the night, on acetazolamide 250 mg since 25th Jan 2022.” However, acetazolamide is not on the supplements/medication list he shares on the Blueprint protocol (link). Is this list just the stuff that he takes for health and longevity? What else is he taking that is not included in this list?
There is one video of him measuring his brain activity using his Kernel device while on ketamine. I would not be surprised if he were actually on psychopharmaceuticals as well.
Concluding thoughts
I overall like Bryan and, as far as I see it, much of his protocol is sound. However, there are a number of things I disagree with:
- He pushes a regime of caloric restriction and having ultra low bodyfat levels, which have severe negative effects on mood, energy and vitality and questionable positive impact on overall health and longevity (with vanity possibly playing a greater role than longevity).
- He overstates his success in combating aging (e.g., through his reliance on erroneous aging clocks).
- He is misleading in that the products he sells have little to do with the results he obtained. More specifically, he is suggesting to the public that many of his results are due to his particular and particularly restrictive diet (part of which he also started to sell) while not commenting so much on the dozens of prescription drugs he is taking.
- Many of the metrics he uses are questionable (e.g., presenting potentially faulty sleep data).
- And worst of all, he overstates how healthy he is. He does not publically discuss his weaknesses (e.g., heart, joints and tendons) and is thus misleading the public about his true health status. Boldly, he even unethically claims “near perfect health”, which is bullshit as already his vital signs are pathological (e.g., body temperature of below 35 C). (Unethical because, firstly, he started to generate money from Blueprint and, secondly, because there are seemingly a bunch of people who are trying to emulate him without understanding the consequences.)
I also disagree with the complete sacrifice of biological vitality for a small gain in terms of longevity – which though is a matter of personal preference.
Bonus: A couple more thoughts on Bryan’s caloric restriction
As of 2024, he is eating roughly 2200kcal per day, which to some may seem far from “starvation”. When it comes to starvation, it is all about relative rather than absolute energy intake. For example, a person who runs a marathon a day would soon be in “starvation mode” on a diet below 4000+ kcal/d whereas some people who just sit on the couch all day may get by fine with only 1500 kcal/d. Bryan engages in a very intense exercise regimen, has very low body fat levels and therefore great insulin sensitivity (i.e., he can tolerate more carbs as his nutrient-partitioning is presumably excellent), and also takes a very high dose of thyroid hormones. In sum, he would probably need around 3000-4000kcal for proper maintenance of his body weight (without his nervous system desperately having to shut down sympathetic activity).
It is true that caloric restriction (CR) is one of the most tested and proven methods to extend lifespan. In fact, next to rapamycin, it is the only method that has been shown to extend lifespan in pretty much every species studied so far. However, these studies are done in sterile labs and not in the wild. Furthermore, pretty much no study was done on very long-lived animals.
Multiple lines of experimental evidence suggest that CR works much better on smaller animals than on larger ones. For example, a 25% reduction in calories can cause mice to live about 30% longer, but only 10-15% longer for dogs. Theoretical models predict minimal to no lifespan extension in large animals such as elephants and whales because in these there are presumably already many adaptations in place that favor a longer lifespan. Likewise, human lifespan may not be extended at all by CR. In fact, data from CR studies on much shorter-lived primates show that CR may not extend lifespan in primates at all. Some markers of health improved but that was about it (and corticoatrophy was observed).
Furthermore, rapamycin (of which Bryan takes quite a high dose) is a powerful caloric restriction mimetic with incredible effects on lifespan and health span in every animal thus far studied. Many of its benefits are most likely due to impacting similar key nutrient sensing pathways compared to caloric restriction. As does metformin and acarbose, which Bryan takes at the highest clinically approved dose. Layering all of these is probably quite superfluous as the results are most likely much less than additive. But it sure does not hurt, so why not? Actually, it probably does hurt.
Given that Bryan gets most of the longevity benefits of caloric restriction by pharmaceutical manipulation, in Bryan’s case, the side effects of caloric restriction (e.g., poor wound healing, faster neurodegeneration, immunosuppression) and the year-round maintenance of starvation levels of body fat may actually be net harmful. They cause his pallor, his hypothermia, and presumably also his obsessiveness. Furthermore, they definitely do not help his bad heart markers and various tendon issues, whether there is a causal role at play is hard to say. All of this does not even include the effects on quality of life – feeling cold, hungry, tired, and “like shit” all the time.
So why does Bryan not increase his calories and gain weight? Presumably because once you have an eating disorder (and large parts of your identity hinge on your looks) it is hard to stop.
Sources & further information
- Article: Blueprint Protocol
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.