
Being at a low bodyfat is metabolically healthy and aesthetically pleasing. However, the price to pay is a decrease in energy, libido, wellbeing, mental flexibility, ever-present hunger and an evolutionary adaptive obsession with food. This decline in vitality and adaptation to starvation is almost single-handedly mediated by the decline in leptin levels, which scale with body fat levels.
With metreleptin one can get the metabolic and aesthetic upsides of being low bodyfat, without the ravenous downsides. And I claim that metreleptin is currently the only way to do this (GLP-1 agonists help here only partially – discussed later) – short of one-in-a-thousand genetics.
Experimenting with leptin was among the most interesting experiments I have ever done. This stuff is powerful and why it is not widely known (or used) is beyond me. It is weird that big pharma has not captured even a fraction of its therapeutic value other than in the ultra-rare orphan disease niche of lipodystrophy.
Furthermore, leptin is completely flying under the radar and I have never encountered a doctor who looks at leptin levels – not even endocrinologists or other hormone specialists. In my opinion, many unsolved problems with energy levels and hormone problems may be due to undiagnosed hypoleptinemia. Many try testosterone and thyroid replacement but still suffer from some symptoms of hypogonadism or hypothyroidism. Even if said hormones are normalized artificially, many of the symptoms remain if leptin levels are low.
Particularly intriguing is that bodybuilding has not got hold of it yet. A bodybuilder’s main purpose in life is pretty much being muscular while being at a low body fat (i.e. being “ripped”). Many of them suffer constantly and battle a ravenous appetite, fatigue, etc. They inject all kinds of anabolic steroids, insulin, growth hormone, and use all sorts of pharmaceuticals for all sorts of purposes. So using leptin too would be a no-brainer. At low physiological doses, immunogenicity is a non-issue and the only downside is the cost and availability, which though are big hurdles at the moment.
Quick background.
Leptin is a master control hormone that regulates long-term energy homeostasis. Leptin is not just a “satiety hormone” as many people wrongly assume, but leptin’s main role is to act as a “starvation signal” when leptin levels are low.
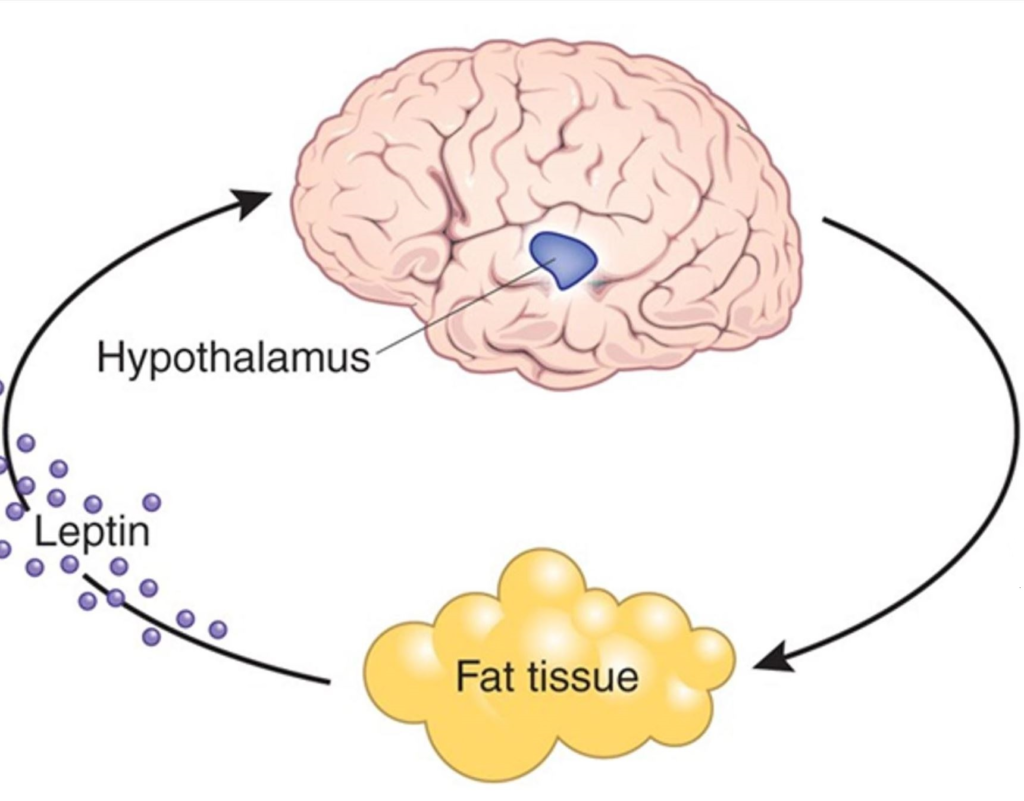
We are the only primates that have conspicuous fat deposits year-round, particularly females (e.g., buttocks, breasts). And when these fat deposits run low, our bodies evolved to shut down many physiological and mental processes. The signal for how “full” these fat deposits are is mediated by leptin. Therefore, leptin can be considered the body’s “fat report” as it is secreted by adipose cells in proportion to how “full” these cells are.
When leptin levels are adequate, this is a “go-ahead” signal for the animal to spend its energy in pursuit of other things besides acquiring food.
When levels get low, all aspects of the organism are driven toward the maintenance of sufficient fat stores for survival. This includes a shutting down of endocrine systems, reproduction, sympathetic nervous system activity, and non-food-related interests. At the same time, appetite, foraging behaviors, and a mental preoccupation with food are all ramped up.
It makes little difference whether leptin levels are “normal” or “high”, but it makes a huge difference if leptin levels fall below a specific threshold, progressively adapting the organism to starvation the lower leptin levels get.
Leptin receptors are expressed in a variety of tissues and organs, including the liver, immune system, and gastrointestinal system. Leptin receptors are even found on the tongue, more specifically taste buds, so that for a starved animal sweet foods taste even sweeter (regardless of leptin also influencing the hedonic response to foodstuff at multiple levels in the brain), which I find fascinating.
However, the major action is on the central nervous system. Leptin receptors are expressed all over the brain and when leptin levels are low, emotions, thoughts, behaviors, and the endocrine system are put into “starvation mode”.

Personal experience
A few years ago I dieted down to very low levels of body fat, which I stupidly maintained for quite a long time.
Even though I had been happy, well-rounded, and sociable, I started to become more unidimensional, withdrawn, secluded, obsessive, rigid, and anhedonic. I also had zero energy, always cold hands and feet, and brain fog. I had no “punch” anymore. I laughed rarely.
I was always lethargic, and it felt like somebody had pulled out my batteries. I had to use cold showers and stimulants just to function. I also had problems with thermoregulation, my mood and libido were low, and simply moving around felt like an onerous task. Over time, I became less physically able, and getting through the day was often a chore. I developed hormonal problems. My mental health took a hit.
I became a pale semblance of my former self. But I did not care much, as being lean had become sort of an “addiction” and something I identified with.
Furthermore, despite the lethargy, I was also quite restless, driven, and my mind was racing all of the time. I was plagued by an inability to sit still and had an irresistible urge to always be productive (presumably a proxy for “foraging behaviors”).I also became socially anhedonic and wanted to be left alone. A lot of my mental brainpower was taken up by food.
I was also quite obsessed and restless: Anecdotes From the Most Obsessive Period of My Life
I had to exercise vigorously every day just to feel normal. Vigorous exercise was one of the few things that reliably lifted me out of the “like shit” state, a state I knew all too well. This was a major reason I trained as much as I did. It was not discipline, it was self-medication, presumably because the exercise jolted my sympathetic nervous system and cortisol into action for a few hours.
I was also highly preoccupied with food, which in times of starvation makes evolutionary sense and is a winner takes all.
I looked the way I wanted to but it came at a price I did not consider before. In fact, the price was everything else. It had consumed my mind, my emotions, my personality, my present moment wellbeing, my hormones, my health. It also consumed my emotionality. Now, I felt nothing. No butterflies when interacting with girls. For me, the only thing that would increase emotions were various pharmacological agents (caffeine, ephedrine, modafinil)…or food.
This might be an okay deal for “fitness influencers”, whose whole life revolves around looking in a certain way, which is fine if you derive 100% of your income and self-worth from it, but for me it was not worth it.
To counter my issues with energy, mood, vitality, low blood pressure, and other adaptations to starvation, I started to replace other hormones (first testosterone, then thyroid hormones, then cortisol), though this only partially helped.
I started to assume that my problem was threefold:
- Low levels of body fat
- Insufficient caloric intake
- Chronic trophic damage done from having been in this state for quite some time
After doing some research, I started to get interested in leptin biology.
My hypothesis was that my leptin had collapsed and with it everything else collapsed. My testosterone, my thyroid hormones, my cortisol, my sympathetic nervous system tone. The rigidity, restlessness and obsession were the neurocognitive aspects of it. My body had entered a state of chronic energy-deficit signaling, a biochemical famine.
I was eager to test out this hypothesis, predicting that that leptin is the thing I needed – whether naturally through body fat gain or artificially through injection. I opted for the latter – partially because my addiction to leanness was a mental disorder.
Procuring a stable leptin supply was a huge hassle (very expensive; very rare) but when I really wanted something I did not stop before I got it. So, soon after making this my mission, I got hold of a stable supply of metreleptin.
At the time, my leptin levels were below 1 ng/ml (hypoleptinemia).
I remember my first time as if it were yesterday. I slept at my girlfriend´s place (she knew all about it) and in the morning I injected a “trial dose”. About four hours later, the colors were more vivid as if imperceptible veil had been lifted. I felt weirdly present and any lingering “heavy limb” sensation and background hunger was strongly reduced. Over the course of a couple of days, I simply felt near normal and knew immediately that “this is it”. I knew there would be an effect but I did not think that it would be anywhere this rapid.
Initially, my dreams were very vivid (presumably because neuroplasticity increased) and my sleep duration increased from 6 hours to about 9 hours for the first couple of weeks. I did not feel energized or motivated, I simply felt normal.
Leptin fully removed the background hunger and the “feeling like shit” (which semaglutide did only to a certain extent), fully normalized my hormone systems, increased my sympathetic tone, and eliminated much of the additional obsession.
For the first time in a long time, I felt somewhat “normal”. Furthermore, I did not have these “distinct-feeling-like-shit” periods anymore during which I was ravenously hungry, restless, and just felt ill. Some effects were immediate (e.g., hunger, “feeling like shit”, thermoregulatory ability, restlessness) and others took more time to develop, such as an increase in energy levels, mood, libido, and emotionality.
Before starting metreleptin, I experienced hunger every few hours, even while taking semaglutide as semaglutide cannot exert its effects well if leptin levels are low – as explained in more detail in my article on semaglutide. However, from the first day of using metreleptin, my post-meal fullness improved significantly – I was able to eat and then stay satisfied for many hours.
In other words, GLP1-agonists help with satiety. Leptin helps with satiation. This means that on semaglutide, I feel satiated quite quickly but if I have low body fat (=low leptin levels) I get hungry soon after. On the contrast, on metreleptin I get the feeling of satiation. I can eat something, and not get hungry for hours.
I was surprised by the rapidity of the effects, which were in fact immediate.
Before metreleptin I had to use a couple of drugs to quite effectively dampen the neurobiochemistry of starvation:
Each single one of these when I first tried them was incredible and I felt great for a couple of weeks. However, eventually, each single one of them got much less effective over time and eventually many of the beneficial effects pooped out. This is something that is common to many interventions. The honeymoon period on TRT or bupropion. The strong simulation on T3. The fantastic effects of moclobemide.
However, metreleptin was different. For the time I was on it, it never seemed to poop out and its effects were mostly sustained, which is further proof that I was correcting a real deficiency. In fact, leptin replaced all of these interventions – and more.
Leptin basically took the body fat issue out of the equation and on it, my 8% body fat functioned like 20%.
Sure, leptin never fully removed all of my symptoms in the same way gaining body fat did but it was the closest thing I have ever tried.
The upside of having gone the artificial route (i.e., injecting leptin) vs. simply gaining body fat was first and foremost that I did not have to gain body fat (remember that I had a disorder). Furthermore, increasing leptin levels endogenously takes time and is very gradual, so having gone the artificial route has allowed me to experience the sharp contrast from low to high leptin levels within a couple of days. Because this was so much “in my face” it really drove home not just the importance of leptin but also the huge costs of my disorder.
As explained in “What Kind of Antidepressant Should I Choose”, depression means a marked downward deviation from baseline. By this definition, whenever my leptin levels were low, I was markedly depressed. And metreleptin was a fantastic antidepressant that worked quite rapidly.
Initially, the dependence was absolute. If I skipped even a single day of leptin, the “feeling like shit” would come back within 24 hours. I lost my vitality and was just 50% myself. Inject again, and the symptoms would lift within a couple of hours.
After a few months on metreleptin, this changed. At roughly the same body fat, or even slightly lower, I could skip a day entirely and feel nothing. The dependence had loosened.
More telling, the effect of leptin got stronger over time (e.g., I lost nearly all of my appetite and nothing seemed appealing and I needed to eat a lot more to maintain my body fat), not weaker, so I repeatedly needed to lower my dosage. This is the opposite of what you would expect from a drug, where tolerance and diminishing returns are the norm. It suggested that leptin was not just filling a gap each day but actually changing something in my brain, presumably reversing stubborn gene expression changes and/or potentiating or weakening certain circuitry.
On the physical side, I noticed was some fat redistribution. Despite not having lost body fat (I actively tried not to by elevating my caloric intake to well above 3000kcal/day), fat redistributed from the facial & trunk regions to my extremities, something that is both metabolically and aesthetically pleasing.
Adipose tissue specifically in my face decreased to the point where many of my friends & family commented on it, particularly my jawline became more pronounced, though my cheeks started to look a little gaunt. Metreleptin-induced loss of facial fat is also reported in the medical literature. Overall, my face became significantly more attractive (as judged by female friends and short-term dating success). Before, whenever I gained weight, a lot of it went to my face. Now, my pattern of fat distribution changed from trunk/face to more extremities.
The leanness of my body finally started to match the leanness of my face. Before metreleptin, my face had always been more chuby than the rest of my body, something that I have seen time and time again in people who had eating disorders (or analogous staes) in the past, because if leptin levels are low, fat is distributed in a Cushingoid fashion, namely disporprotionately to the fat and face.
Replacing leptin essentially lowered my “fat setpoint”, allowing for maintaining very low body fat levels without suffering from lethargy, ravenous hunger, hormone deficiencies, and other starvation-related adaptations, which would obviously be of immense value to the modeling, acting, fitness, and bodybuilding industry.
Overall, it took many months of normalized eating, weight gain, and leptin exposure to feel mostly again – probably accompanied by measurable brain changes in a number of regions. Leptin receptors are widely expressed in the brain, and the brain adapts as a consequence of prolonged starvation/undereating. In some sense, this adaptation allowed humans evolutionarily to “prime” their brain, hormones, and metabolism for further episodes of starvation. By putting myself in a normoleptinemic state artificially, it is plausible that most of these brain changes, which had presumably trophically and epigenetically adapted to “starvation mode”, reversed back to “normal mode” by the constantly ongoing high leptin levels. There is fMRI evidence that after 1 year on metreleptin, there are a number of trophic changes in brain structure.
I ended up taking a low dose of metreleptin for 4 years, which were some of the best years of my life. Furthermore, during these years my personality started to change and approach my adolescent personality to some extent. For example, I became quite balanced and decently emotional again. My obsession and neuroticism declined to low levels. The rigidity went away almost completely and I got more flexible, well-rounded, and much less stingy.
I started to care about others again. I wanted to spend time with them and they wanted to spend time with me because my energy and mood normalized. I was finally able again to do things again purely for the sake of enjoyment (e.g., reading in parks, going for walks, etc.) and not because they had an obvious productive aspect to them. It was fascinating to witness what a sustained signal of abundance did to my nervous system on all fronts. So, all in all, my life was the best and most balanced it has been in over a decade.
When I was on leptin, my fasting insulin levels were always below baseline (because my insulin senstivity was so high) and on a DEXA scan I only had 66g of visceral fat, which is essentially nothing. Furthermore, even low doses of leptin made it nearly impossible to gain body fat even if I tried. I became “that guy” that could eat whatever he wanted without ever gaining an ounce of body fat.

There are a ton of people who do “everything right” but their body fat will hardly go below 15%. Conversely, there are others who can eat whatever they want and they are constantly under 10%. With metreleptin I was in the latter category. Years ago I gained quite a lot of fat by eating 2500kcal per day. On metreleptin, I needed to eat above 3000kcal in order to not lose weight, while at the same time having a body fat of roughly 9%.
Because overeating in a state of very low appetite is a huge nuisance, and I wanted to gain fat, I decided to decrease my dose of metreleptin progressively. I started to gain fat literally immediately and overall my body gained about 5% body fat (from about 9% to 14%) within a couple of months, even though I did not change what or how much I was eating.
So, this molecule was definitely doing something “deep” to my energy homeostasis.
While procuring the drug was a hassle, playing around with metreleptin was one of the most interesting and fruitful experiments I had ever done. I may write a more detailed article about my experience with metreleptin at some point in the future as this is something that, to my knowledge, nobody has done (or at least written about) before. To get notified when it is available, sign up for my newsletter.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
How does leptin work?
Leptin is an adipokine – a cytokine derived from adipose tissue.
Leptin has a lot of effects on all kinds of tissues. For example, it instructs the liver to store less fat and therefore reduces visceral adiposity. It also instructs muscle cells to burn more fatty acids for energy. It acts on a plethora of immune cells making them “sharper”. It increases insulin sensitivity in liver, muscle, and fat cells, which together comprise more than 80% of someone´s body mass.
However, the most important effects are on the brain, where leptin acts on a variety of brain areas. In fact, leptin is a master control hormone and whenever it is low, the whole nervous system is severely affected. Leptin acts at many sites in the CNS. This includes not just the hypothalamus (discussed shortly), but also the VTA neurons (producing dopamine), the raphe neurons (producing serotonin), the hippocampus (where leptin increases neuroplasticity), the insula (having to do with interoception), the anterior cingulate cortex (a lot of things pertaining to emotions), and others.
Mechanistically, leptin is a membrane-receptor hormone acting through the JAK-STAT cytokine-signaling pathway that is directly linked to powerful gene expression changes.
As mentioned above, leptin receptors are expressed in a variety of tissues and brain sites but the most important of these sit in the hypothalamus.
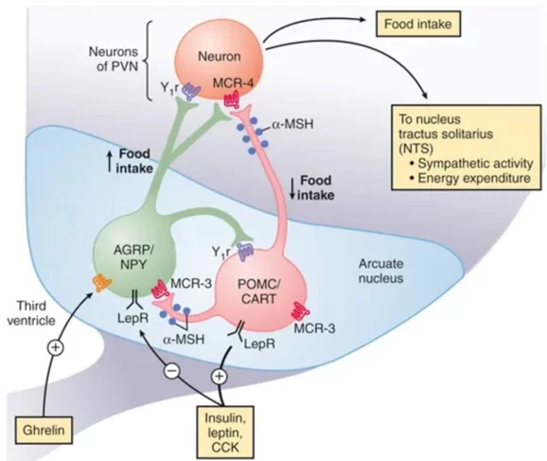
Below is a graphic of POMC/CART and AGRP/NPY neurons in the ventromedial nucleus of the hypothalamus. I won’t go too much into the science aspects of it but these neurons are ultimately responsible for telling the rest of the brain and body that there is sufficient energy availability to spend in pursuit of things other than food. These neurons are a major target of leptin. In fact, leptin is needed for them to be active.
Very briefly: The decrease in leptin signaling results in the downregulation (suppression of activity) of a group of hypothalamic POMC neurons that are responsible for signaling to the brain that the organism has sufficient energy availability. At the same time, there is an upregulation of a second group of neurons (so-called AgRP-neurons) that are important for mediating the effects of energy deprivation. These neurons are central to neuroendocrine and autonomic control, and whenever their activity is turned upside down (decrease in POMC-neuron activity; increase in AgRP-neuron activity), a lot of bodily systems are gradually shut down and people start to feel cold, hungry, weak, and are preoccupied with thoughts about food.
POMC/CART and AGRP/NPY neurons are ultimately responsible for telling the rest of the brain and body that there is sufficient energy availability to spend in pursuit of things other than food. They do this by a variety of mechanism:
- By co-controlling hormonal output of the anterior pituitary gland (HTA, HPA, HTPA). Hence, many “fit” individuals have hormone issues involving all three major axes. This is also the main reason that women lose their period if they are calorically deprived or lose weight. The before and after of this is well described in the literature in patients with congenital leptin deficiency or hypothalamic amenorrhea when they are given leptin injections.
- By regulating sympathetic activity, the latter of which is the major regulator of energy expenditure. Hence, many people with low body fat are feeling weak, have low blood pressure and a low heart rate. In combination with the decline in hormones, this is the main reason people start to lose energy and feel drained as they lose weight.
- By affecting appetite and nudging certain brain areas to think about food-related stuff. Hence the constant background hunger and obsessive eating habits. This is also the main reason people get more hungry as they lose weight. This obviously makes evolutionary sense. Quoting a lipodystrophy study: “In the leptin-deficient state, the current study patients anecdotally described an addiction-like affinity with food, with large parts of their free time revolving around food preparation and consumption. After a meal, satiety only persisted for ∼1 h. After metreleptin treatment, patients experienced longer periods of satiety after a meal, reduced meal frequencies, and lost interest in thoughts about food.”
- By upregulating dopaminergic neurotransmission – hence the restlessness and drive/obsession that is commonly seen in starving animals and restrictive eating disorders. If mice are starved and a running wheel is put into their cage – they paradoxically run themselves almost to death (presumably a proxy of foraging behavior). If you then inject leptin, these mice stop running.
- By affecting various areas in the nervous system (e.g., the anterior cingulate cortex, insula, amygdala etc.) that affect behavioral, cognitive, and emotional patterns (aka personality) in a way that makes people more likely to pursue and acquire food. Hence, some people became more self-centered, rigid, and stingy – presumably traits that are intended to help with hoarding and foraging behaviors. The phenotype of this is well described in the Minnesota starvation experiment.
- By influencing thermoregulatory processes. Hence, the pale complexion because the body centralizes blood flow. Furthermore, this is also the reason that some only feel comfortable within a narrow temperature range and having issues with sweating (thus heat intolerance) and heating up (thus cold intolerance).
For me, leptin made a world of a difference in all of these domains pretty much overnight: energy levels, mood, libido, restlessness & obsession, rigidity, thermoregulatory ability, appetite levels, sleep, cognition, and emotionality.
These changes were much more powerful than the changes I experienced with semaglutide. It turns out that these neurons also express receptors for GLP-1 and semaglutide was activating them to some extent, which is the primary reason GLP-1 agonists are so damn effective for weight.
However, leptin is the background modulator of POMC-neuron activity and without enough leptin (i.e., low body fat levels), GLP-1 agonists do not work properly and/or do not turn them on as fully as leptin does. I discuss the science of this in more detail here: The Syndrome of the Ultra Fit
How does leptin differ from GLP-1 agonists?
GLP-1 agonists turned out to have the effects people always hoped leptin treatment would have. The catch with leptin is that at high body fat it does not work well, partly because of “leptin resistance” (though it is not clear this is even a real phenomenon), and partly because leptin signaling is already close to saturated – adding more does little.
GLP-1 agonists sidestep this and activate the POMC-neurons described above. Interestingly, they also seem to sensitize cells to leptin, as evidenced by the fact that leptin receptor expression increases on GLP-1 agonist treatment. On top of that, they have many leptin-independent effects of their own.
But the relationship runs both ways. At very low body fat, when leptin levels are low, GLP-1 agonists themselves stop working well, because they appear to require adequate leptin signaling to exert their effect. This is exactly where GLP-1 agonists fail and metreleptin becomes the tool you actually need.
So the two drugs are mirror images. GLP-1 agonists work when body fat (and leptin) is high and fail when it is low. Leptin does the opposite. Between them, they cover opposite ends of the body-fat spectrum.
Furthermore, when leptin levels are low and leptin is given, leptin has many more effects on neurobiology. It strongly influences energy levels, mood, and reverses neurocognitive adaptations to starvation, such as obsession, restlessness, rigidity, and anhedonia.
At the receptor level, GLP-1 agonists act on a GPCR (mostly linked to acute changes in cellular activity) whereas leptin acts on a cytokine receptor (mostly linked to longer-term changes due to directly affecting gene expression).
The graphic below illustrates that the lower leptin levels (red bar), the stronger the effects (blue bar) if leptin is given. And the higher the leptin levels (common obesity) the weaker leptin is.
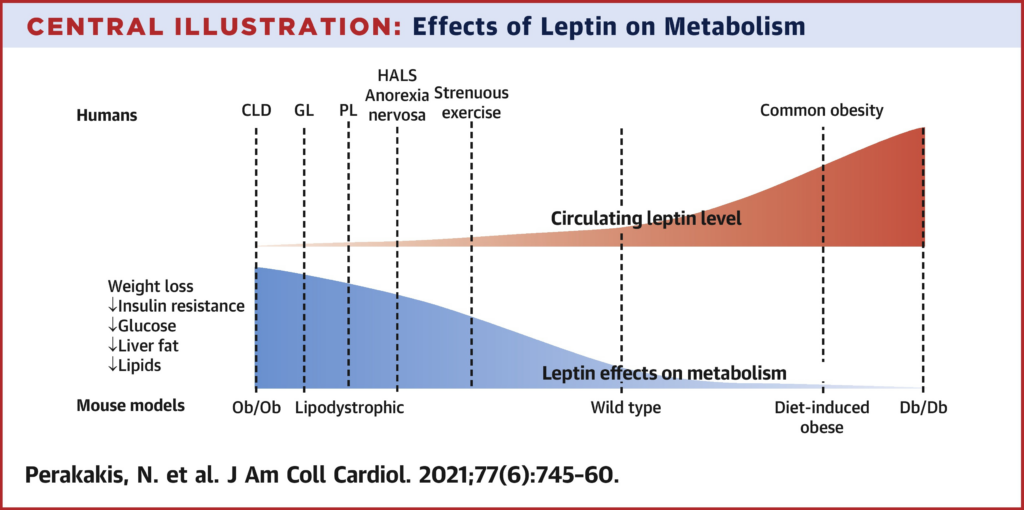
(CLD = congenital leptin deficiency; GL = generalized lipodystrophy; PL = partial lipodystrophy; Ob/Ob = leptin mutants)
Leptin regulation
The more fat you carry, the more leptin you produce.
That is the simple version, and it is roughly right. But the devil is in the details.
Low levels of body fat cause low levels of leptin. However, whenever fat stores are actively diminishing, levels of leptin decline even more (regardless of baseline level of body fat). Furthermore, diets low in insulin (esp. fasting, very low carb diets) cause the most extreme decline in leptin levels -and the decline is even greater than the combined decline from low levels of body fat and the (independent) decline from actively diminishing fat stores.
Leptin secretion does not simply track the number of fat cells. It tracks how full each one is. A large, well-stocked fat cell secretes disproportionately more leptin than a small, depleted one. This has a consequence that matters. Thus, doubling your fat mass can more than double your leptin. And in reverse, as those cells empty out, leptin drops faster than the fat does.
The relative collapse at low body fat
In absolute terms, leptin changes more per percentage point of body fat when you are heavier. Going from 30% to 25% body fat might drop leptin by several ng/mL, while going from 10% to 5% drops it by only a couple. So in raw numbers, the curve is steeper at the top.
But your body does not respond to raw numbers. It responds to proportions. And proportionally, the picture inverts:
- 20% → 15% body fat might take leptin from ~6 to ~4 ng/mL. That is a drop of roughly 33%.
- 10% → 5% body fat might take it from ~2 to ~0.7 ng/mL. That is a drop of nearly 66%.
Same five-percentage-point change. Radically different biological signal. Going from 9% to 7% body fat can cut leptin in half. The same absolute fat loss starting from 25% barely registers.
An analogy: losing €5,000 when you have €100,000 in the bank is an inconvenience. Losing €5,000 when you have €7,000 is an emergency. Your hypothalamus does not care how many nanograms of leptin disappeared, it cares what fraction of the signal vanished.
This is why the consequences of getting very lean arrive so abruptly rather than creeping in gradually. It is also why athletes, bodybuilders during contest prep, and patients with anorexia nervosa end up with leptin levels near zero, and with the whole downstream cascade that follows: suppressed hormones, absent libido, obsession, low energy, cold intolerance, relentless hunger, and preoccupation with food.
Leptin also tracks energy intake
Leptin does not only report fat stores. It also reports whether energy is currently coming in. This happens partly because insulin stimulates leptin secretion, and partly because leptin tracks glucose flux through the fat cell directly. Eat carbohydrates, and leptin goes up within hours. Stop eating, and it falls within a day, long before you have actually lost meaningful fat.
The same person at 10% body fat might show:
- ~2 ng/mL while weight stable and eating normally
- ~0.5 ng/mL after several days of aggressive caloric restriction
- ~3 to 4 ng/mL after a couple of days of carbohydrate overfeeding
That is a sixfold to eightfold swing, with essentially no change in how much fat they are carrying.
This is the mechanism behind the “refeed” or “carb-up” that lean athletes swear by. It is not that a big carbohydrate meal restores fat mass, it obviously does not. It is that it temporarily restores the leptin signal, and the brain, which cannot see your fat directly and only reads the hormone, briefly stops running the starvation program.
Of note, all the values above are rough figures for men. Women have roughly two to three times higher leptin at the same body fat percentage, driven by differences in fat distribution (more subcutaneous fat, which has a larger effect on leptin) and sex hormones (testosterone directly lowers leptin expression independent of its effects on body fat).
The summary
Leptin is dependent on multiple variables:
- How much fuel is in the tank (fat stores): This has the strongest and most direct effect on leptin levels.
- Whether the fuel stores are actively changing: When fat stores are actively declining (e.g., fasting), leptin drops disproportionately. Similarly, when fat stores are actively increasing (e.g., refeeding period) leptin levels rise disproportionately.
- Carbohydrates: Insulin and glucose flux are both independent variables that affect leptin secretion. This is the weakest of the three.
At moderate body fat and a normal caloric intake, all signals are comfortably intact and small changes are tolerable. At low body fat, the two most important variables can collapse at the same time, a small further loss of fat causes a large proportional drop, and any dip in food intake compounds it. This is why the low end of the body-fat range behaves like a cliff rather than a slope, and why the physiology changes so much below a certain treshold.
Symptoms of low leptin levels
- hormone imbalances
- low energy levels
- low sex drive
- ravenous appetite
- reactive hypoglycemia
- restlessness
- low sympathetic nervous system activity (e.g., low blood pressure, low heart rate, low body temperature, fatigue)
- persistent symptoms of multiple hormone deficiencies that do not adequately improve with hormone replacement therapy
Diagnostics
- Blood test: leptin
Interventions that worked for me and friends
- Metreleptin: The only currently available leptin analog. Mibavademab, a leptin receptor agonizing antibody, is currently in clinical trials though it is uncertain whether brain sites beyond the circumventricular organs are reached.
- Gaining body fat: Body fat levels are the major determinant of leptin levels. At low body fat levels, leptin levels are low. However, high body fat levels are often accompanied by leptin resistance. Most males feel and function best between 13-18% body fat even though they look the best around 10-14% body fat, on average.
- Semaglutide: Semalgutide is a known “leptin sensitizer”, which means that leptin signaling is potentiated. Among other things, GLP-1 agonists are thought to increase the expression of leptin receptors on the order of 40-70% but presumably also enhance intracellular leptin signal transduction. Of note, for me, metreleptin allows me to keep my body fat low without starvation-related adaptations, something that semaglutide does not.
- Increasing caloric intake: It seems that caloric intake has an effect on leptin levels independent of body fat levels. Furthermore, it seems that a high caloric intake has a leptin-sensitizing effect in the hypothalamus, regardless of body fat levels.
- Increasing carbohydrate consumption: Insulin potentiates leptin synthesis.
- Avoid: ketogenic diets, intermittent fasting, multi-day fasting, dieting
Where leptin could be helpful
Leptin essentially fools the body and brain into thinking that it has more body fat than it really has. This may be helpful in a number of medical condition and “lifestyle” departments.
- Hypothalamic amenorrhoe
- RED-S (relative energy deficiency syndrome)
- Anorexia nervosa
- Recovery from prolonged yoyo-dieting
- Bodybuilding
- Modelling/Showbusiness/Acting
A note on Anorexia Nervosa
Exogenous leptin is possibly also an unintuitive way to treat anorexia nervosa, the most severe form of restrictive eating disorders.
The development of anorexia can be thought of as a two-step process. Firstly, an individual wants to lose weight and embarks on a pursuit of thinness, usually for control and/or aesthetic reasons. This is the psychological step. Secondly, after an individual gets down to very low body fat levels (and only people with an iron willpower ever will), leptin levels tank which causes many of the adaptations of starvation to set in, which then causes people to become OCD-like, obsessive, rigid, and inflexible. These neurocognitive adaptations basically make people even more obsessed with whatever their goal is goals (in case of anorexia – the pursuit of thinness). In fact, the inability to change goals may be how the “entrapment” in anorexia nervosa happens and this starvation-related biological exacerbation of obsession may possibly be central to the pathogenesis of anorexia nervosa.
Thus, once leptin levels tank, a huge biological component is added to the picture and this biological escalation (second step) makes the psychological fixation on thinness (first step) much worse. In a way, it closes the cage.
Unintuitively, leptin administration in this state may help in a number of ways:
- Firstly, it dissects the psychological from the biological components of the disorder and removes the neurobiological starvation state, which presumably lessens the obsession and rigidity associated with the disorder, which over time allows for the building of new habit and thinking patterns and helps with setting new goals. In a way, leptin administration makes patients are finally amenable to psychotherapy, which untreated anorectics are notoriously resistant to.
- Secondly, spending an extended period of time in a leptin-replete state reverses many of the long-term trophic brain changes happening in starvation (“imprinting”) resulting in the gradual reversal of the metabolic, endocrine, and neurocognitive adaptations of the disorder. This is analogous to how antidepressants work: They change brain chemistry acutely and also in the long-term and therefore help people to build their life back up.
- Last but not least, metreleptin normalized fat distribution patterns. In anorexia or other eating disorders, fat gain happens in a Cushingoid fashion, namely, disproportionately to the face and trunk, which is one of multiple reasons why so many people relapse after weight gain because they cannot stand the way they look. Normalizing fat distribution could make the needed fat gain less distressing to patients, possibly lowering relapse rates.
Together, this would make exogenous leptin a potentially promising candidate treatment that could serve as a bridge between disorder and normality in a similar way antidepressants can serve as bridge between depression and normal life. The risky aspect is that leptin fools the brain into thinking “I have more body fat than I actually do” which increases basal metabolic rate. Thus, if not paired with adequate caloric intake it could be abused for further weight loss. But barring the risk of abuse, leptin administration could potentially help a lot of people in their mental, physiological, and aesthetic recovery.
Anyway, despite the risks, this is a hypothesis worth testing and my startup set out to do so.
Leptin vs. ghrelin?
There is a widespread misconception that leptin is the antagonist of ghrelin. This misconception implies that leptin and ghrelin play in the same league of importance. Nothing could be further from the truth.
Leptin is one of the few master control hormones, whereas ghrelin serves a few highly specific and to some degree expendable minor functions, exerting its effects on measly G-protein-coupled receptors. Leptin, on the other hand, exerts its effects via a special cytokine receptor, directly linked to widespread and major alterations in gene expression through STAT3 activation.
If ghrelin would be gone from one second to the next, not much would happen. However, if leptin is gone, the whole organism is on fire. For more, google “congenital leptin deficiency”.

“I can maintain sub 10% body fat with no issues”
The human body evolved a mechanism that it stops working properly if adipose tissue reserves are too low, presumably for survival-related reasons. However, purely from a functional perspective, there is little reason to assume that humans need to carry more fat than the closely related chimpanzees.

Even though carrying a decent amount of adipose tissue is not needed from a functional perspective, the human body nonetheless evolved to “shut down” when adipose tissue is lacking by way of gradients in leptin signaling.
Every one of us has a different “leptin threshold” level and also a different level of leptin synthesis for a given amount of body fat. Furthermore, individuals differ in terms of leptin sensitivity. Consequently, some people can naturally stay at very low levels of body fat without adverse effects, whereas for others body fat needs to be much higher.
There are a couple of people who claim that they can maintain a sub 10% body fat “just fine”. I suspect that the vast majority of these people are either purposefully lying, have little self-awareness about how much body fat they actually have, or are so much used to their state that they have simply forgotten what being in “normal non-starvation mode” feels like.
Obviously, there are genetic differences in leptin secretion per fat mass and/or leptin receptor signaling and some people can truly stay at very low body-fat levels without suffering from starvation-related adaptations – but the vast majority of people cannot.
To test this, if somebody can truly maintain a sub-10 % body fat level “just fine” (or sub-18 % for females), he would not feel anything from metreleptin administration at a dose sufficient to mimic 20% body fat.
Unfortunately, many people do not really recover after dieting down to a body fat level too low (e.g. cold intolerance, anhedonia, loss of libido, lethargy) – online there are many anecdotes of people that seem to have permanently screwed themselves by dieting down too low. Even more unfortunate, leptin agonists (which are next to impossible to get hold of) are perhaps the only thing that can truly reverse these changes without a significant amount of fat gain.
I discuss this in more detail here: The Syndrome of the Ultra Fit
The dangers of keeping body fat % too low
Even super fit males lose all their energy once their leptin starts to drop – they turn into zombies with less energy than unfit, overweight, old people. A couple of quotes I have taken from Reddit about people discussing their experience with maintaining very los levels of body fat:
- “I did not even have the energy to change TV-program.”
- “Some days being super lean I remember driving home from work or the gym and wouldn’t even have the energy to buckle my seat belt I would just let the car keep beeping.”
- “In general, I’ve found that if I drop below about 8%, I start to lose my libido and my energy levels plummet.”
- “Never stayed single digits for very long. Always felt very drained, not with it and performance is shit. Personally feel good at low to mid teens.”
Or Zac Efron after filming Baywatch: “I started to develop insomnia, and I fell into a pretty bad depression, for a long time. Something about that experience burned me out. I had a really hard time recentering. Ultimately they chalked it up to taking way too many diuretics for way too long, and it messed something up.” Well, it was not the diuretics but the profoundly low leptin levels that messed him up.

I recently dated a woman who has had amenorrhea for over 2 years. She also had cold hands and feet and a blood pressure of 105mmHg. Her SHBG was high. She felt tired most of the time.
Endocrinologists did not know what was wrong with her because releasing-hormone tests had shown that her hypothalamus and pituitary functioned perfectly well when diagnostically stimulated with releasing-hormone tests. She even went to the best university endocrinologists (which should know about hormones) which even sequenced her genome.
Sometimes you do not need fancy genome sequencing or complex releasing tests as they are often inferior to a well-done health history in conjunction with knowing about physiology.
She told me that a couple of years ago she had lost about 15kg of fat. Ever since, she maintained this weight through willpower. Why no endocrinologist (one of them a university professor) has picked up on that important detail is beyond me. The role of leptin in hypothalamic amenorrhoea has been well-known for a long time (study).
Similarly, about a decade ago, I dieted down to single-digit body fat levels (4.8% at my lowest point) and stayed around there for about a year (perhaps the biggest mistake I have made in my life). I did this mostly because of vanity reasons. Back then, my energy levels were abysmal and multiple hormonal axes were in the gutter. My mental health was much worse as well.
Weight regain and starting to eat 3000kcal/d have not fully reversed all of the starvation-related adaptations even years after the fact. Supraphysiological doses of “satiety” peptides (insulin; GLP1-agonists; metreleptin) mostly normalized things though only while I was taking them. As soon as I came off, many of the adaptations came back.
Of all the interventions I had tried, leptin administration was by far the most powerful.
After weight recovery, former patients with anorexia nervosa have all sorts of issues for a long time – even if they recover more than their original fat mass. For example, in one study, baseline noradrenaline levels as well as stimulated noradrenaline levels remained much lower even 4 years after weight recovery.
Similarly, after the biggest loser study, participants had a negative delta in their basal metabolic rate of about 500-600kcal per day (!) despite being back to their original fat mass. The only hormone that was much lower 7 years after the fact was lepti (study).
It seems, that the brain somehow “remembers” periods of starvation (whether self-induced or otherwise) and that, for many people, these adaptations are quite stubborn and hardly go away in a similar way obesity hardly goes away after a person has become obese. (Of note, GLP-1 agonists only lower body weight/fat setpoint while the treatment is ongoing but as soon as people come off, most of the weight is regained).
How does this “imprinting” happen? There are two possibilities (at least, I cannot think of any other). Firstly, adaptations happen at the level of neural networks (long-term depression or long-term potentiation of existing networks). Secondly, adaptations happen at the cellular level (perhaps sustained alterations in the expression of certain transcription factors in key neuronal populations such as POMC/CART neurons presumably due to gene methylation).
In sum, maintaining body fat much below the fat set point for a long time seems to carry long-term risks. Some regain their weight and recover fully and quickly. Others are not so lucky. I have met quite a few people who did not recover properly – some did not even recover after becoming much fatter than they were.
I discuss this in much more detail here: The Syndrome of the Ultra Fit
The importance of body fat
The following is a copy&paste of the last two sections of my article on semaglutide. I feel that it fits here well too.
For me, the introduction of semaglutide into my system eliminated that hard-to-fight urge to constantly eat. The feeling of true satiety, which I had not experienced in a long time, became my new normal state (and I soon got used to it).
Initially, I lost some weight, but as my body fat approached single digits, the feeling of hunger and weakness returned. Even though a small meal would now satiate me quite quickly because of semaglutide, I nonetheless got hungry quite soon after eating. Self-experiments with metreleptin have shown me that this was due to low leptin levels.
It seems that leptin has a permissive effect on semaglutide action, meaning that if leptin levels are too low, semaglutide does not work properly. The reason is probably that leptin signaling is coupled to a cytokine receptor (STAT3 signaling) paving the way for POMC neuron activity whereas semaglutide signaling is only coupled to a measly GPCR receptor.
Weight and appetite regulation are based on two things:
#1: Energy intake
When energy intake remains below caloric needs, weight-gain-favoring adaptations occur. Energy levels, mood, sex drive, satiety, etc. all take a hit – regardless of body fat levels. Caloric intake is signaled to the hypothalamus by a plethora of mechanisms. These include satiety-peptides (GLP-1, CCK, PYY, PPY), insulin, vagal nerve endings from the gut, stomach stretch, and even hypothalamic receptors for glucose, fatty acids, and amino acids. GLP-1 agonists can partially hack this (which is why they are so effective for weight loss), meaning that GLP-1 agonists mimic “food abundance”.
#2: Body fat
When levels of body fat are low (individuals vary with regard to what “too low” means), adaptations to starvation will be set in motion regardless of energy intake. This is single-handedly signaled by the adipokine leptin, which is secreted by adipose tissue in proportion to how “full” an adipose cell is. This means that if body fat levels (more specifically, leptin levels) are below a certain threshold, the rest of the satiety system ceases to work properly. Unbeknownst to many, the effects of leptin go far beyond appetite regulation. I discuss leptin in more detail here.
Therefore, as a member of Homo sapiens, I have to accept that my body fat levels must not be too low and, other than through the administration of a leptin analog, there is no way to circumvent this – at least if vitality and mental sanity are a priority.
The human body evolved a mechanism that stops working properly if adipose tissue reserves are too low, presumably for survival-related reasons.
A brief note on evolutionary biology
When I was a child, I imagined archetypal nature to be this caring, nursing mother. However, as I learned more about the world, it turned out that romantic Mother Nature is rather cruel and callous. The Earth’s biosphere in its original state is incapable of supporting human flourishing as it is naturally infested with predators, parasites, food scarcity, and a variety of diseases.
Given that this was the evolutionary backdrop against which my ancestors’ bodies and minds developed, I now find myself in an utterly unnatural environment. In the same way that humans invented technologies to tailor the biosphere to human flourishing, I can use technologies (e.g., pharmacology) to update my body and mind to the contingencies of the modern world.
For example, in the past, food was usually quite scarce and therefore, my ancestors evolved to be drawn to junk food, overeating, and storing fat. However, this is maladaptive in the modern-day environment. The fact that modern food has been engineered to trigger overconsumption surely does not help either (sweetness; umami; mouthfeel; caloric density; flavorings; crunchiness; etc.).
My primitive brain is therefore mismatched to this modern ecosystem of convenience and abundance and an orchestra of mechanisms wants me to pig out. For many members of my species, food addiction, obesity, type II diabetes, and cardiovascular disease are a consequence.
I use GLP-1-agonists to modify the homeostatic and hedonic aspects of feeding and, in my opinion, using this technology is only as artificial as living in the modern world in the first place.
This also makes me wonder whether we humans are generally unfit for the future in the same way our “thrifty genes” are unfit for the present. Fortunately, the ability to discover and use explanatory knowledge (a.k.a. science) gives us humans the power to transform nature and ourselves – limited only by the laws of the universe.
Why I have not built antibodies to metreleptin
I discuss this in more detail here: Why I have not built antibodies to metreleptin
Sources & further reading
- Scientific study: Short-term metreleptin treatment of patients with anorexia nervosa: rapid on-set of beneficial cognitive, emotional, and behavioral effects
- Scientific review: The role of hypoleptinemia in the psychological and behavioral adaptation to starvation
- YouTube: Tristyn Lee – My Experience Maintaining 4% Body Fat for 2 Years