
Metabolic health is intricately connected to everything. For this article, I want to give credit to Dr. Peter Attia. I learned more from his podcast The Drive than from my biochemistry classes.
What is metabolic health?
It is hard to define what metabolic health is. It is easier to define it by what it is not. Metabolic health is the opposite of metabolic syndrome, which is essentially a disruption in proper energy metabolism. In practice, metabolic health is somewhat synonymous with “being highly insulin sensitive”, which has to do with a myriad of different factors ranging from muscle mass, exercise status, inflammation, and a plethora of genetic and hormonal factors, some of which are discussed in more detail shortly.
Metabolic health is a continuum. At one end, there are highly metabolically healthy individuals with great insulin sensitivity, metabolic flexibility, and nutrient partitioning. On the other end, there is full-blown type 2 diabetes.
In the industrialized world, currently, around 10% of the adult population is suffering from type 2 diabetes (but only about half are aware of it). Due to an aging population, more sedentary lifestyles, and increasing adiposity, the prevalence of this disease is expected to double within the next twenty years or so. Many more people are currently prediabetic and/or have “metabolic syndrome”.
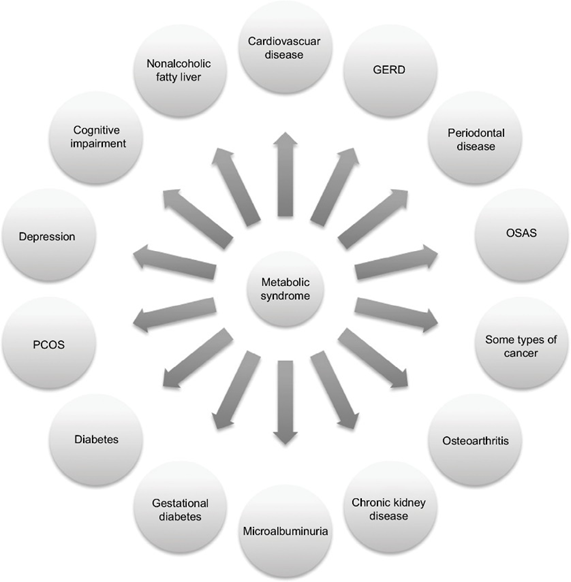
Someone is “diagnosed” with metabolic syndrome if they have at least three of the following:
- hyper-glycemia
- hyper-tension
- hyper-lipidemia
- hyper-weight
Down the line, most people with metabolic syndrome will end up with serious conditions such as heart disease (including heart attack and stroke), type 2 diabetes, chronic kidney disease, cancer, or dementia.
Together, these constitute the most common causes of death worldwide. Metabolic syndrome was also one of the most important underlying factors that caused people to succumb to COVID-19, which illustrates the importance of metabolic health for health and longevity.
Metabolic health depends on a number of things. These include genetics, exercise status, a variety of different hormones, muscle mass, and body fat levels (particularly the amount of visceral adiposity). These factors can tilt metabolism towards a more healthy or a less healthy state.
Tactics I follow to promote metabolic health
- Muscle mass
- Endurance exercise
- A note on VO2 max
- Hormone optimization
- Metabolic drugs
- My experience with fasting
- (Mostly) avoiding sugar
- Thoughts on carbohydrate intake
- (Mostly) avoiding dairy
- Occasionally wearing a CGM
- Sleep optimization
- Thoughts on omega-3 & omega-6 fatty acids
- Keeping body fat levels low
- Leptin
- Supplements
- Are drugs necessary?
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Muscle mass
I try to maintain a decent amount of muscle mass. To do so, go to the gym a couple of times per week. Muscle mass is fundamentally acquired by progressive overload and a slight caloric surplus. Obviously, I “never skip leg day” because legs have by far the biggest muscle groups in the body (at least in humans). My TRT Lite protocol surely helps.
Having a decent amount of muscle mass is known to improve every aspect of metabolic health. Muscle is a very insulin-sensitive tissue that will function as a “glucose sink”, therefore improving insulin sensitivity and nutrient partitioning. The more muscle, the more glucose and fatty acids are mopped up by muscle tissue at rest, particularly during the hours post-workout.
Therefore, all else being equal, more muscle equals greater insulin sensitivity.
I discuss the effects of exercise on vitality (energy levels & mood) in more detail here.
Endurance exercise
Zone II exercise is cardiovascular exercise performed right at the cusp before lactate starts to accumulate. Said another way, it is exercise during which oxidation of fatty acids is at its maximum. Through a variety of signaling pathways, zone II exercise stimulates mitochondrial function and mitochondrial biogenesis, which vastly improves metabolic health through a variety of mechanisms.
A couple of times per week (depending on the season) I do a dedicated session of zone II cardio. Below is a screenshot from my Polar data of what a zone II session looks like for me (I usually end with a 5min high-intensity part). My average heart rate is between 70-80% of my maximum heart rate (which is a little over 180bpm).

A proper endurance exercise session is known to improve insulin sensitivity for at least 24 hours. I am always amazed at how potent this is when I look at my CGM data. For example, eating pizza after a heavy endurance session has much less of an effect on my blood sugar compared to eating pizza without having exercised that day.
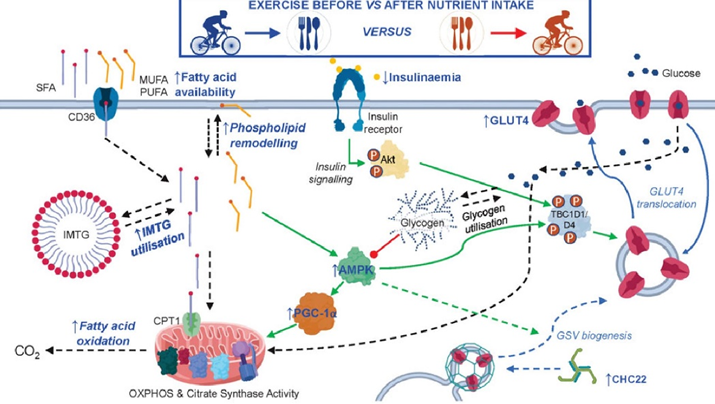
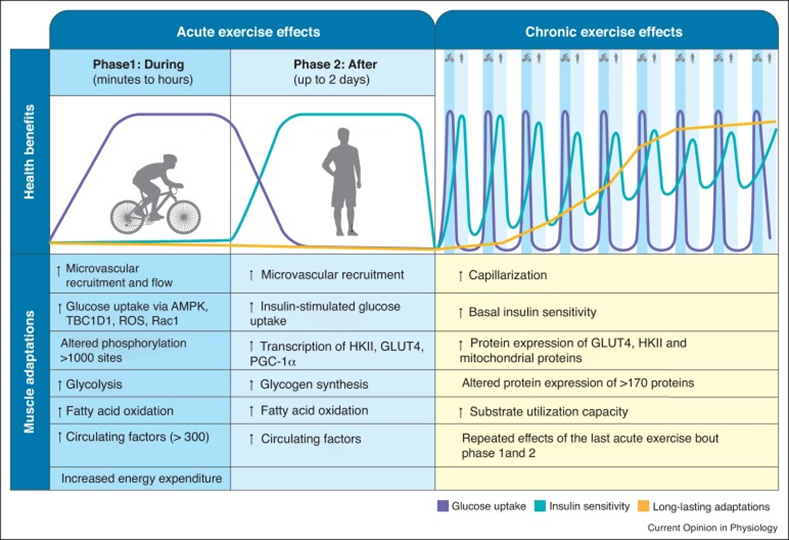
Exercise, in particular endurance exercise, leads to countless adaptations in skeletal muscle. One of the presumably most important changes is an improvement in mitochondrial function and stimulation of mitochondrial biogenesis. Said another way, endurance exercise increases both the number as well as the quality of mitochondria, which have a variety of positive effects on metabolic health (and a number of other things).
Furthermore, endurance exercise stimulates an insulin-independent GLUT-4 translocation, which will reduce blood glucose levels in an insulin-independent way.
Moreover, endurance exercise leads to a depletion of intracellular nutrient stores (particularly glycogen), which activates a metabolic master switch enzyme called AMPK with downstream effects of increasing insulin sensitivity.
On an epigenetic level, endurance exercise also leads to altered expression of a large number of genes.
Because of these changes, a single endurance exercise session increases insulin sensitivity for many hours to come.
Furthermore, by regularly depleting glycogen stores (e.g., by regularly doing endurance exercise), dietary glucose is handled the way it should be, namely, by being funneled into hepatic or muscle glycogen synthesis. Conversely, if glycogen stores are always tapped out, excess glucose is biochemically much harder to manage and comes with a host of unfavorable biochemical alterations.
In sum, the end result is that endurance exercise has an incredible effect on insulin sensitivity and mitochondrial function, both of which are at the center of metabolic health.
A note on VO2 max
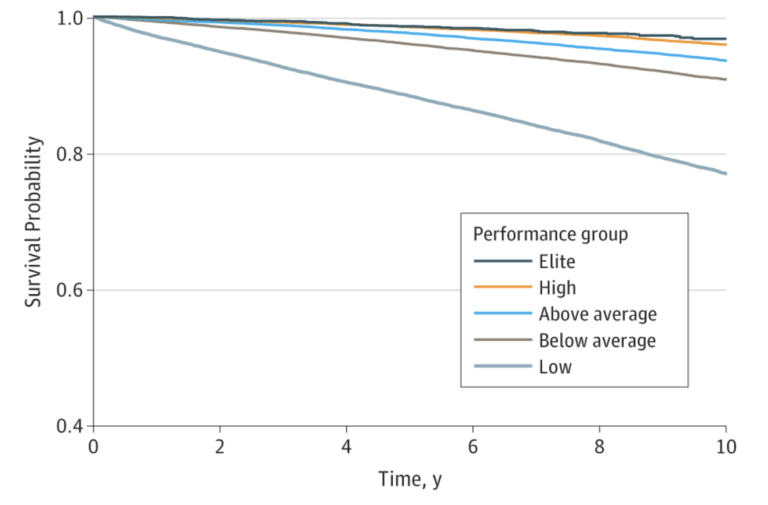
VO2 is a measure of how much oxygen (and therefore metabolic substrates) my muscles are capable of using during physical exertion, which is an indicator of how well mitochondria are performing. VO2 max is highly correlated with lifespan and health span, as “survival of the fittest” would predict.
According to Peter Attia, the “ideal” VO2 max training is spending 80% of the time allocated to aerobic exercise in the zone II range (about 75-80% of maximum heart rate) and spending 20% in zone V (e.g., via HIIT training). According to Dr. Attia, the minimum effective dose is about three hours per week.
I end most of my cardio sessions with a 5-minute high-intensity part. I do not do more because I hate HIIT.
Hormone optimization
I watch a number of hormones closely, including sex hormones, thyroid hormones, and IGF-1. Having “youthful” levels of these hormones will improve nutrient partitioning, insulin sensitivity, muscle growth, keep body fat reasonably low, and hundreds of other things.
Furthermore, hormones have powerful effects on energy levels, mood, vigor, and vitality, and therefore, they make leading a healthy lifestyle much easier.
Currently, I only supplement with HCG and a low dose of metreleptin.
Metabolic drugs
For multiple years, I took a low dose of semaglutide. I mostly used semaglutide to reduce my appetite, which I find distracting. Semaglutide has significantly increased my quality of life. I discuss my experience with it in more detail here. For the past 2 years I have been off it because it lowers my appetite too much, even at very low doses. weight gaining impossible.
For most people, semaglutide increases metabolic health because it leads to a loss of body fat, which increases insulin sensitivity. Some people worry that it decreases muscle mass. Personally, I have built about 5 kg of muscle on semaglutide, though I also started doing CrossFit at about the same time.
Because my levels of uric acid are generally on the higher end, I also take allopurinol (150mg/d) to reduce my uric acid to the 4-5 mg/dl range.
In the past, I have also experimented with acarbose, metformin, and SGLT-2 inhibitors, but for me, all three had more downsides than upsides. I am currently also off rapamycin, which undoubtedly affects (improves?) metabolic health.
I discuss a variety of metabolic drugs, and my experience with them, in more detail here.
Fasting
Intermittent fasting and multi-day fasting are both known to improve metabolic health through a variety of mechanisms. For example, both are known to reduce mTOR activity and upregulate AMPK activity, improve insulin sensitivity, stimulate autophagy, and promote metabolic flexibility.
As always, many processes happen in parallel and a plethora of changes are cross-interacting, influencing, and driving each other. Parallelism is something our brains are just awfully bad at grasping because we evolved to cognize linearly in space and time.
However, for me, all kinds of fasting did more harm than good. I discuss my experience with intermittent fasting here, and my experience with multi-day fasting here.
Mostly avoiding sugar
A couple of years ago, I was low-level addicted to sugar, in particular chocolate. Interestingly, since going on semaglutide it seems that sugar, and sweetness in general, has lost most of its “pleasure” (though, I can still taste it normally – just without much “pleasure”). Interestingly, this effect persisted even after coming off semaglutide.
Sugar in the way it is currently consumed, is addictive and causes weight gain and creates all sorts of metabolic issues. Fructose metabolism significantly differs from glucose metabolism, often leading to intrahepatic fat accumulation, which then drives insulin resistance, metabolic disease, and obesity.
Obesity comes down to two things:
- 1) People eat too much (e.g., due to boredom, psychological eating, constant availability of highly palatable foods rich in fat & sugar & salt).
- 2) People store too much (regardless of how much they eat).
By hijacking the reward system (“people eat too much”) and causing insulin resistance (“people store too much”), sugar hits both.
Interestingly, on a diet high in fructose, many people get insulin resistant and develop a fatty liver (NAFLD) even if they do not gain weight. Likewise, many people have a dramatic improvement in metabolic health & NAFLD if they simply switch out fructose for glucose. For this very reason, some researchers call fructose “ethanol without the buzz”, as it leads to non-alcoholic-fatty-liver disease (NAFLD) in a similar way alcohol leads to alcoholic fatty liver disease (AFLD).
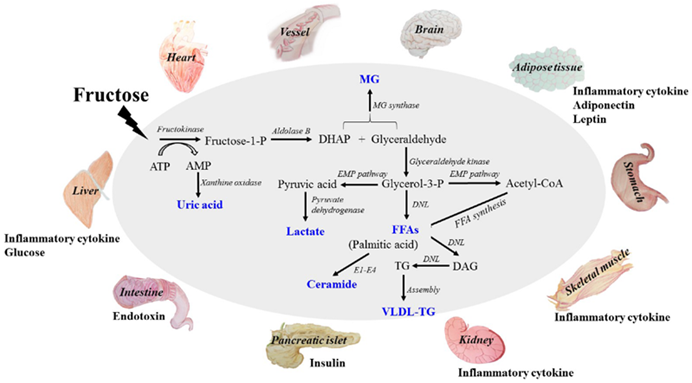
Furthermore, fructose is thought to elevate levels uric acid levels, which not only elevates blood pressure but also seems to crystallize in the form of calcium urate crystals, gradually over decades leading to low-level organ damage (much more than just gout).
What about fruit? Consuming fruits in reasonable quantities is probably fine as the fructose contained is not very concentrated. Furthermore, there is an adequate amount of fiber contained within most fruits, which slows stomach emptying and enzymatic breakdown. As a result, lots of the fructose in fruit is metabolized to glucose in the intestinal tract long before it can overrun the liver.
Blockers of fructose metabolism are currently in clinical development by Pfizer.
I discuss sugar in more detail here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Avoiding alcohol
In terms of metabolic health/disease, ethanol is quite similar to fructose. It worsens metabolic health and leads to intrahepatic lipid accumulation, which causes insulin resistance.
Furthermore, alcohol worsens sleep, which is also important for metabolic health because firstly, the nervous system regulates cortisol secretion (which has dramatic effects on metabolism) and secondly, the nervous system regulates body weight and insulin secretion.
I find that already the slightest amount of alcohol destroys my sleep parameters (SWS, REM, RHR, HRV, body temperature patterns), at least as measured by my Oura ring. I used to party a lot when I was younger but at this point in life, “sacrificing” the next day is not worth it anymore. I only drink it on very special occasions but then I really enjoy it.
Carbohydrate intake
I feel and function best if I titrate my carbohydrate intake to my leanness and activity levels. So, usually, I eat quite a lot of carbs (about 300-400g per day) because I simply feel and function better if I eat them. I find that if I do lots of strenuous activity (e.g., CrossFit) I can tolerate a lot more carbs because they are immediately burned (or absorbed) by muscles.
Similarly, the leaner I am, the more carbs I need to not experience a decrease in energy levels. This is likely because insulin is “the hormone of abundance” and signals to various brain nuclei (first and foremost hypothalamic POMC neurons) that there is no reason to worry about starvation.
I believe that low-carb diets are great for people who are overweight and/or metabolically deranged, but they may do more harm than good for people who are already lean and insulin-sensitive.
I discuss my approach to macronutrients in more detail here.
“Bad” carbs
In the past, I tried to “hack” this by using acarbose or SGLT-2 inhibitors, both of which reduce post-meal glucose excursions. However, acarbose consistently spiked my liver enzymes and SGLT-2 inhibitors consistently dehydrated me. Needless to say, I stopped taking both. I do not worry too much about “bad carbs” but I mostly avoid overly sugary carbs.
Dairy
For many people, dairy may be inflammatory, drive gut issues, and seems to negatively affect the lipid profile and metabolic health. This might be due to some of the protein fractions in diary (i.e., whey & casein) being hormonally active (i.e., possibly, they are transcytosed and act on hepatocytes).
I personally eat a lot of dairy, sometimes exceeding 2l of whole milk or kefir a day, which is my favorite drink of all time.
I discuss dairy in more detail here.
CGM
From time to time, I carry a continuous blood glucose monitor (CGM) to see whether my diet needs some changes. Below is a screenshot of a day that went particularly well.
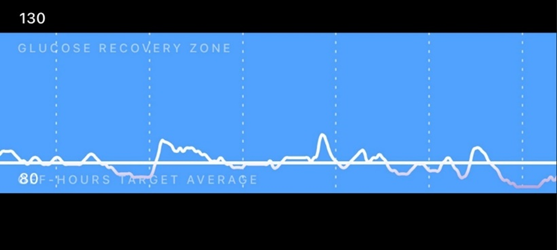
Through CGM use, I found out that I am very insulin sensitive, and on self-performed OGTTs I am back to baseline after about 20-40 minutes (usually undershooting my baseline slightly). I attribute this to my leanness and high activity levels.
Sleep optimization
There are multiple ways in which bad sleep hampers metabolic health.
- In a sleep-deprived state, cortisol levels are generally high. Cortisol has a huge effect on various aspects of metabolism. In Cushing syndrome (excess cortisol levels) metabolic health is usually crap.
- Good sleep is necessary for proper growth hormone release. Growth hormone is anabolic to muscle and catabolic to fat, particularly visceral fat (discussed shortly).
- The nervous system itself is quite a powerful regulator of metabolic status. For example, through vagal nerve endings, the nervous system affects liver metabolism and insulin secretion. Bad sleep is usually associated with greater basal insulin secretion, likely independent of cortisol and presumably mediated by vagal control of the pancreas.
- In a sleep-deprived state, willpower and metacognition are poor, which leads to bad food choices and forgoing exercise, both of which are causally related to metabolic health.

I discuss how I optimize my sleep in more detail here.
Omega fatty acids
Omega-3: I make sure I get enough Omega-3 fatty acids. I supplement with 2g of EPA/DHA per day. I describe them here.
Omega-6: While the science is inconclusive, it seems that high amounts of omega-6 fatty acids may promote inflammation by being converted into pro-inflammatory prostaglandins. Therefore, some researchers believe that it is best to avoid excessive consumption of vegetable oils (e.g., soy, corn, sunflower) because of their high omega-6 fatty acid content. I find this to be a huge nuisance in modern life, and I pay little attention to it. I wish food manufacturers would just switch out sunflower oil for canola oil, which would (likely) make our lives a little healthier.
Keeping body fat levels low
One of the most powerful interventions to improve metabolic health is to keep body fat levels low. I personally keep my body fat in the 10-12% range and measure my body fat once in a blue moon via a DEXA scan. I discuss body fat in more detail here.
Tools I use for keeping body fat low include exercise and a very low dose of metreleptin. The addition of a low dose of metreleptin allows me to keep a low body-fat percentage without suffering from starvation-related adaptations.
The less adipose tissue there is, the more “primed” adipose cells are to store fat, and the lower the adipose tissue-mediated inflammation. This means, that all else being equal, a lower body fat percentage is associated with less inflammation, better insulin sensitivity, and improved nutrient partitioning. The vast majority of people with little adipose tissue have decent to great metabolic health (some Southeast Asian ethnicities may be an exception).

In particular, ectopic fat (fat stored in non-fat cells) and visceral fat (fat stored around the liver) is the metabolic devil, causing inflammation and insulin resistance. Both are highly correlated with increased levels of obesity. And since visceral fat is, for the most part, a function of body fat percentage, keeping body fat levels low is one of the most effective ways to prevent visceral fat accumulation.
Visceral adiposity leads to a fatty liver, which wreaks havoc on all aspects of metabolic health, particularly insulin sensitivity. The science is quite complex and has to do with local adipokine signaling, the local elevation of free fatty acids activating the inflammasome, and free fatty acids inducing insulin resistance. I discuss visceral fat, and potential ways to reduce it, in more detail here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Leptin
Leptin is a very misunderstood hormone. It has little to do with being “the satiety hormone” as it is commonly believed. Rather, the purpose of leptin is to protect the animal from starvation. Because my body fat is lower than my body would like it to be (about 10-12%), my leptin levels are naturally very low (less than 1ng/dl).
Leptin has a huge effect on metabolism. Firstly, it is a master-regulatory hormone that affects hypothalamic and pituitary function on a broad level. In a state of hypoleptinemia, hypothalamic functions such as thermoregulation, sleep, sex drive, energy metabolism, appetite, sympathetic nervous system activity, and hormone secretion are all affected in a way to prime the organism to conserve energy and to store fat.
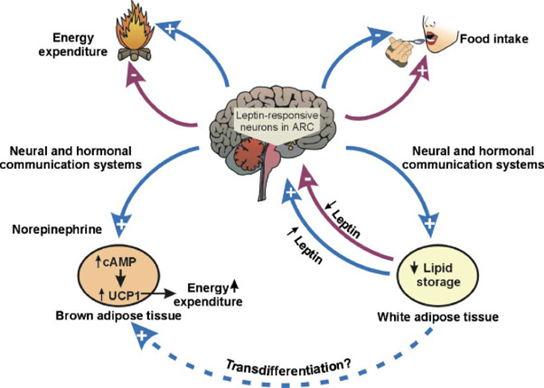
Secondly, leptin acts directly on the liver, adipose tissue, and muscle cells, among others, instructing them to alter intracellular metabolism. For this reason, leptin analogs or leptin receptor agonists are promising interventions to treat non-alcoholic fatty liver disease. Hypoleptinemia may also be the reason why some lean and healthy individuals sometimes have erratic blood sugar patterns and some other metabolic (and hormonal) issues.
Leptin expression and secretion are highly correlated with the amount of adipose tissue someone carries, particularly subcutaneous adipose tissue.
To increase my endogenous leptin secretion (without gaining weight), for a couple of months in the past I have topically applied a self-made cream containing the PPAR-gamma agonist pioglitazone (which induces preadipocyte differentiation) to my upper legs with the goal of increasing the number of local subcutaneous adipocytes to preferentially shift fat storage towards this region. I did this to create my own endogenous “leptin factory” in a place that is optically not displeasing.
Ever since my upper legs have now a slightly thicker layer of subcutaneous adipose tissue. As a side note, I suspect that pioglitazone cream could potentially become the next anti-aging cream because of its ability to counteract, and perhaps even reverse the age-associated loss of facial fat. Unfortunately, my leptin levels only rose barely or not at all.
I decided to hack my way around gaining fat by jumping on a very low dose of metreleptin sufficient to mimic a body fat percentage of 20% (but without the aesthetic and metabolic downsides of actually being 20% body fat). Interestingly, from that point on my blood glucose became much more stable (among many other things).
The mental changes were profound. I plan on writing an article about this in the future.
Using metreleptin allows me to carry a lower-than-ideal body fat percentage without any soul-sucking starvation-related adaptations (e.g., mood, energy, sex drive, sleep, hormonal health) while benefiting from the aesthetic and metabolic-health-improving effects of having low body fat.
It is no rocket science to infer that leptin agonists could potentially revolutionize bodybuilding and a fitness industry focused on being “shredded”.
I discuss leptin, and my experience with it, in more detail here.
Supplements
I am quite sure that compared to the other tactics on this list, supplements do comparatively quite little. Most of the supplements I take are taken with a “just-in-case” mentality, and I am equally uncomfortable taking them compared to not taking them. Nonetheless, I have been taking a variety of supplements for about 4-5 years now, and nothing “bad” has happened.

I discuss the supplements I take, and why I take them, in more detail here.
Are drugs necessary?
It might be obvious by now that I have a fondness for pharmacology. However, I am pretty sure that I (and presumably most other young healthy people who have not been overweight during childhood or adolescence) could achieve pretty decent metabolic health by lifestyle changes alone, including a hefty dose of exercise, keeping body fat levels fairly low, eating healthy, avoiding sugar, avoiding dairy, and optimizing sleep.
However, some of the same signaling cascades that are activated by lifestyle choices can also be manipulated pharmacologically. In principle, my cells could not care less whether downstream signaling pathways are activated by lifestyle choices or pharmaceutical intervention.
I discuss my thoughts on the “ethics” of intervention in more detail here.
For a variety of reasons, I choose to take metabolic drugs even though they are not necessarily necessary. All five drugs I regularly take are, to some extent, metabolic drugs. These include thyroid hormones, semaglutide, metreleptin, allopurinol, and rapamycin. However, these drugs are by no means a replacement for the lifestyle changes discussed above.
Other articles
Because metabolic health is a huge (and hugely important) topic but this article is already awfully long, I wrote three articles on the subject that will go in much more depth:
For more info on muscle mass & longevity, I highly recommend Outlive by Peter Attia.
My Longevity Protocol (Long & Technical Version)
This article is part of a much larger post describing my complete longevity blueprint. For my full protocol, read here.
Sources & further information
- Podcast:Peter Attia & Richard Miller: The gold standard for testing longevity drugs: the Interventions Testing Program
- Podcast:Peter Attia & Ronesh Sinha – Insights into the manifestation of metabolic disease
- Scientific study:The acute vs. chronic effect of exercise on insulin sensitivity: nothing lasts forever
Disclaimer
The content on this website represents the opinion and personal experience of the author and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without a doctor’s supervision. The content presented is exclusively for informational and entertainment purposes. Never disregard professional medical advice or delay in seeking it because of something you have read on the internet.