
Hormones are crucially important for physical, mental, and emotional health. If even just one of the major hormones is off, optimal well-being, performance, and mental health are not on the cards. When hormones are replaced in a balanced and physiological way, often striking results can be seen within a short period of time.
I discuss some of the major hormone basics and my experience with thyroid hormones, testosterone, cortisol, and leptin in greater detail here.
In this article, I will briefly discuss my experience with various other hormones.
Growth hormone
A couple of years ago, I experimented with growth hormone, mostly out of curiosity regarding how it “feels”. Dosages varied from 0.5 IU to 2 IU per day. For reference, a healthy adult pituitary produces about 1-1.5 IU per day.
For the first couple of days to weeks, there was a distinct feeling of calmness and slight euphoria. My dreams were incredibly vivid. After that, I was unsure whether the GH did anything noticeable. Even at 1IU per day, my IGF-1 levels went up by about 100-150 points, giving me IGF-1 levels of roughly 400ng/dl.
At the dosages I was using, there was little to no water retention, though at the time I was also on a ketogenic diet, which is known to increase natriuresis given that the kidneys are an incredibly insulin-sensitive tissue.
I also tried various GH secretagogues, though I never noticed anything from them. Ibutamoren (MK677), a ghrelin-receptor agonist, made me ravenously and insatiably hungry 24/7 and I stopped it after about 1 week.
I specifically want to mention the effect of GH on sleep. The older one gets, the less REM and SWS and the more stages 1 and 2 (shallow sleep) there are throughout the night. This is partly related to the decline in growth hormone. After I had put my dad on a short course of a low dose of growth hormone, he mentioned how amazing his sleep had become and how rested he felt after waking up. The increase in sleep quality is one of the most common observations after people try growth hormone therapy.
How it works
Similarly to leptin, growth hormone acts on a cytokine receptor, which is directly tied to alteration in gene expression through STAT signaling. These kinds of receptors are much more powerful than measly G-protein-coupled receptors as they directly alter the expression of dozens if not hundreds of genes.

GH receptors are widely distributed and thus growth hormone has many effects in a variety of tissues, including the brain. Roughly 1/3 of the effects of GH come from GH itself but the rest of the effects are indirectly mediated through GH-induced stimulation of hepatic synthesis of IGF-1.
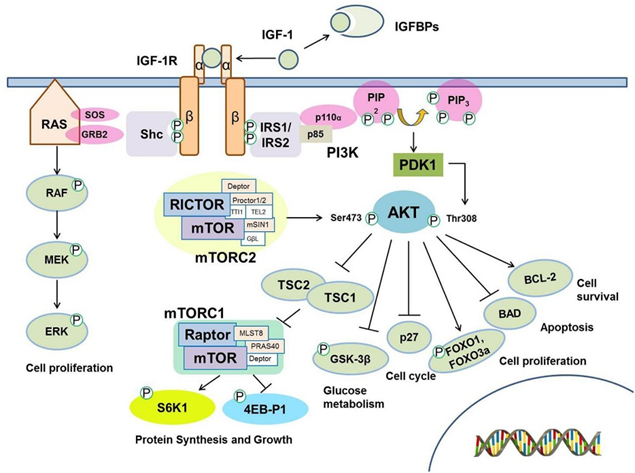
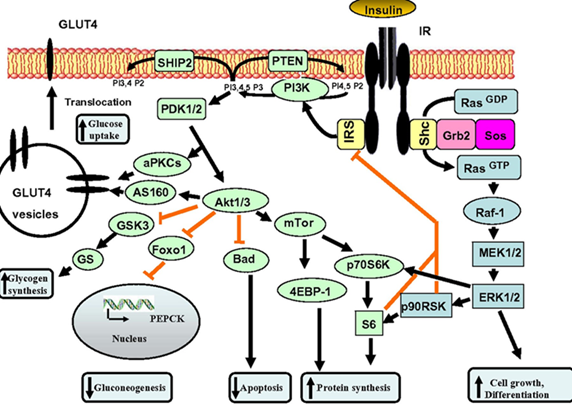
IGF-1 acts on a receptor tyrosine kinase, which is connected to major signaling pathways regulating cellular activity, cellular growth, and proliferation. IGF-1 receptors are found on pretty much every cell of the body and IGF-1 is perhaps the most important systemic growth factor, along with insulin. In fact, insulin and IGF-1 share many overlapping signaling pathways and the two proteins are quite similar in many aspects.
Even though IGF-1 presumably drives the aging process, it is part of the reason why young people heal faster, learn well, grow muscle easily, have more REM sleep, and have a hard time gaining fat. Through its actions in the nervous system, it is also correlated with energy levels, mood, and vitality. There is an inverse relationship between IGF-1 levels and dementia.
While higher levels of growth hormone may reduce absolute lifespan, some anti-aging researchers claim that they may increase practical/average lifespan through their effects on vitality, musculoskeletal health, metabolic health, and cognition.
I discuss the upsides and downsides of IGF-1 in more detail here.
Long-acting insulins
At one point when I was very lean, my fasting insulin was very low (which is good for longevity) and I wanted to see whether adding a low dose of a long-acting insulin would help my energy levels.
I decided to use 5 IU of insulin degludec, which has a half-life of about 30 hours. For the first couple of days, there was a definite increase in energy levels, though even this tiny does wrecked my heart rate variability (decrease of about 20ms or so) and caused me to wake up and be wide awake at around 3 am, which presumably happened because my system was not used to fasting levels of insulin being that high. As discussed above, insulin shares many of the effects of IGF-1.
To lower my night-time insulin levels, I switched to insulin detemir (half-life of about 12 hours) and my HRV and sleep went back to normal. I stopped after about a month or so because I did not feel much different. Blood glucose was about five points lower. Interestingly, my body hair seemed to grow faster.
I repeated this experiment a couple of years later. A clear-cut increase in energy levels for the first week or so and I felt exhausted for a couple of days after stopping it. The same thing again, I noted an increase in body hair growth, which made me stop. My working hypothesis is that because of my leanness, my fasting insulin levels are very low which reduces “growth” of everything.

How it works
Long-acting insulins differ from insulin mostly with regard to half-life. Some insulins are better at interacting with the IGF-1 receptor than native insulin. For example, insulin detemir has a decent interaction with the IGF-1 receptor and would therefore make a good choice for bodybuilding purposes.
I discuss the science of insulin and strategies I use to keep insulin sensitivity high, in much more detail here.
Oxytocin
I have experimented with injectable oxytocin a number of times. The first time, I have taken it was with a very good friend, mostly out of curiosity. We both administered 10 IU subcutaneously. We both felt nothing. However, my blood pressure shot up to 140mmHg which is presumably due to oxytocin interacting with ADH receptors found throughout the vasculature. The next day, my libido was raging.
I also experimented with lower doses (2.5 IU – 5 IU) a couple of times with one of my ex-girlfriends. Starting perhaps an hour or so after, I felt quite warm/butterflies in my stomach and there was a low-level euphoria, though it is hard to say how much of that was due to placebo.
The only thing I could feel for sure was greater libido, greater penile sensitivity, and longer & stronger orgasms, which is in line with oxytocin receptors being highly expressed in genital organs. Hard to explain but sex on it felt magical and everything was just “better”.
I have a lot of pharma grade oxytocin sitting in my fridge but I have not experimented with it in over two years, partly because I have a weird ineffable inner resistance against messing with the human bonding system.
How it works
Oxytocin has both central and peripheral effects. Similar to many other hormones, it is associated with myriads of small effects in many organ systems, though presumably not much would happen if one knocked out the oxytocin receptor (other than in the brain and sex organs).
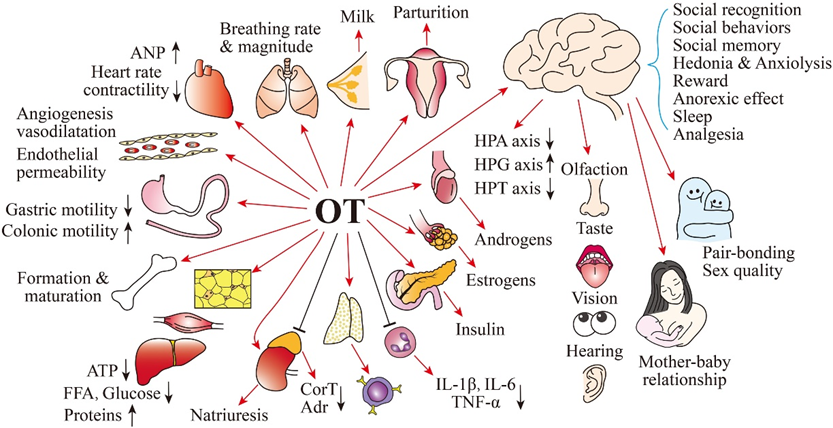
Peripheral effects include, for example, a contraction of the musculature found in the pelvic region. As I was using it, I could definitely feel that my orgasms were longer and stronger, presumably due to this mechanism. However, oxytocin is also thought to increase libido through modulation of the mesolimbic system.
Central effects include a modulation of mood and cognition in a way that facilitates “bonding” with others. For example, In a simulated economic investment game, subjects who received an intranasal spray of oxytocin were more inclined, as compared to a placebo control group, to trust another player by sending him money with no guarantee of reciprocation.
Oxytocin is also famous for increasing both in-group as well as out-group behaviors. Essentially, this means that it makes individuals bond to “kins” but makes people more hostile to “non-kins”. As so often with hormones, the effects of oxytocin are context-dependent.
Oxytocin deficiency has been linked to numerous psychiatric disorders including autism, schizophrenia, depression, and anxiety disorders – though whether there is any causal connection is currently unknown.
ADH (desmopressin)
Out of curiosity, I have experimented with desmopressin to see whether it has some effects similar to oxytocin. Both are nonapeptides important for bonding and other social aspects. All it did was make me retain some water and reduce the number of times I needed to urinate. I also felt some pressure in my head for about 12 hours after taking it, presumably due to increased blood volume.

How it works
In some animals, ADH is even more important than oxytocin for social behaviors. More and more work is coming out that vasopressin abnormalities are frequent in autism and that supplemental vasopressin improves social behaviors of autistic children, much more than oxytocin. In some studies, measuring CFS vasopressin levels was predictive of a future autism diagnosis.
Anecdotally, there are reports that ADH also improves memory retention and recall.
Next to its effects on the brain, anti-diuretic hormone (ADH) is the primary hormone regulating minute-to-minute osmolarity. When osmolarity falls, which largely depends on sodium concentration, ADH is secreted from the posterior pituitary to stimulate renal water absorption through the insertion of aquaporin proteins. When this mechanism fails (e.g., due to low ADH or due to ADH-receptor mutations) diabetes insipidus ensues. ADH also contracts blood vessels.
However, it should be noted, that the osmolarity-regulating functions and social functions of ADH are from a distinct group of neurons. With the former, ADH-secreting neurons are secreting ADH into the bloodstream (ADH as a hormone). With the latter, ADH-secreting neurons are secreting ADH to other neurons in the brain (ADH as a neurotransmitter), similar to oxytocin.
EPO
A couple of years ago I was borderline anemic due to undereating and high doses of rapamycin. Out of curiosity, I used weekly microdoses of EPO (first epoetin alpha and then switching to “super-EPO” darbepoetin) to get my hematocrit up to about 50% just to see whether I would feel any different.
About 2 weeks after my second EPO dose I realized that I just did not get tired and barely out of breath at all while being on my recumbent exercise bike. That was a very fascinating experience. Cyclists and other endurance athletes frequently abuse EPO.
Interestingly, after each microdose, I got a slight headache resistant to treatment with NSAIDs, which was presumably due to stimulation of erythropoiesis within my skull bones.
How it works
On a molecular level, EPO works very similar to growth hormone. Both act on a cytokine receptor and both act through STAT signaling. The major difference is receptor localization and which STATs are recruited after receptor binding, culminating in the expression of different target genes.
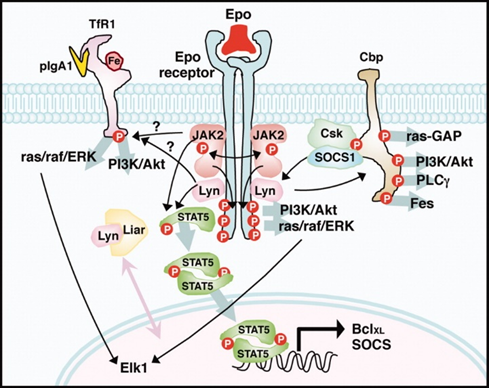
Interestingly, the increase in EPO levels is associated with some of the beneficial effects of SGLT-2 inhibitors. I.e., EPO levels rise quite strongly on SGLT-2 inhibitors.
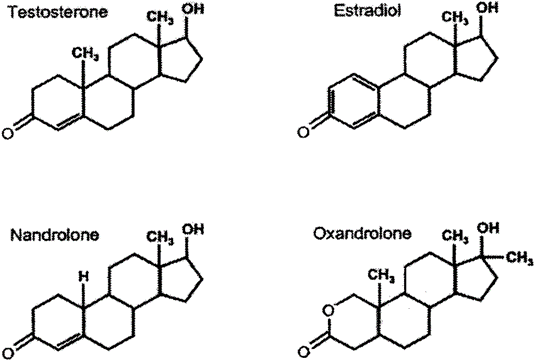
Estradiol
When I was on TRT, I added some topical estradiol to the mix to experience what high estradiol “feels” like. Of note, most of the time estradiol is manipulated in a way to reduce levels (e.g., through aromatase inhibitors), and rarely do people add estradiol.
The first time I experimented with it, I felt overheated and fatigued, which made me stop quite soon. The second time I tried it, I did not notice much, though the doses I used may not have been enough. I switched over to 17-alpha estradiol, which is a tad less feminizing.
On and off, I applied microdoses of topical estradiol to my undereye region to reduce dark circles as estradiol is known to stimulate dermal growth and deposition of subcutaneous fat. Ever since, I feel that my undereye circles are a little better though I cannot say with 100% certainty.

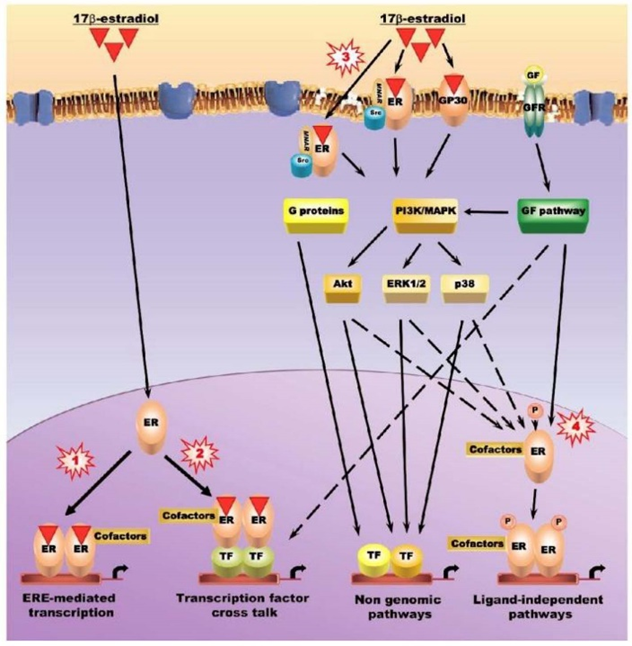
How it works
Similar to other steroid hormones, estradiol acts on nuclear receptors, directly affecting the expression of hundreds of genes. The genes induced depend on whether they are accessible in a specific cell type. For example, estradiol stimulates the expression of different genes in e.g., neurons versus adipose cells.
Estradiol is crucial for a lot of stuff, including metabolic health, brain health, normal levels of aggression and libido, joint and bone health, etc.
The importance of estradiol can be seen when it is blocked (or when women enter menopause). Men typically complain of crushing fatigue, joint pain, absent libido, a reduction in aggression and drive, a drop in mood, and brain fog. In the long run, there is dementia and osteoporosis.

Next to nuclear estrogen receptors, there are also transmembrane estrogen receptors but their functions have not yet been properly determined. Of note, transmembrane receptors also exist for other steroid hormones (testosterone, progesterone) but their effects are presumably minor and expendable in comparison to their effects on gene expression.
Estradiol is interesting because, molecule per molecule, it is perhaps the most potent hormone in the human body. It is only present in minute amounts. A normal healthy male has about 600 nanograms/dl of testosterone but only 3 nanograms/dl of estradiol (usually measured in picograms/milliliter).
This means that molecule for molecule, there is about two hundred times more testosterone than estradiol molecules. Even in women, testosterone outnumbers estradiol by about 10 to 1 (unless they are taking oral contraceptives) – neglecting the cyclical ups and downs of hormone levels.
Of note, estrogen counters some effects of testosterone on a genetic level. For example, topical estradiol can prevent hair growth caused by DHT. For this reason, a friend of mine, who is on TRT, applies low doses of estrogen gel (Estrogel) to his face to prevent testosterone-induced facial aging.
Oxandrolone
A couple of years ago, I experimented with a microdose of oxandrolone (1.25-2.5mg/d) to help with adding some muscle, mostly for vanity reasons.
While bodybuilders might find this dose laughable as they generally use 10-50mg per day (often in combination with other anabolics), on paper, even a 1mg/d dose is quite a decent anabolic boost considering that my natural T secretion is about 8-10mg per day (blood levels of roughly 650-750ng/dl) and oxandrolone has an androgenic-anabolic ratio of roughly 1:6 – meaning that 1.25mg of oxandrolone (anabolic equivalent of about 6-8mg of testosterone) would almost double my exposure to anabolic agents if my endogenous secretion did not decline while taking it (which is a big “if”).
After my first dose (2.5mg) I was incredibly sore for a couple of days after the same gym workout I had been doing for a long time, indicating that something was up with my muscles. In the gym itself, I was much more vasodilated and I looked like somebody who was doing steroids (which I technically was).
I measured my blood levels three times during the three to four months I was on it. Even at this low dose, oxandrolone slashed my LH, total testosterone, SHBG, and free testosterone by about 40%, and, on paper, I was borderline hypogonadal (total testosterone of about 400ng/dl). Interestingly and unexpectedly, my (measured) estradiol did not change much, though I have not used the ultra-sensitive test.
I found that, for me, 2.5mg every other day suppresses my sex hormones much more than 1.25mg every day (50-60% vs. 30-40% suppression) despite the same weekly dosage.
For me, at this dose, there were no discernible effects on liver enzymes and blood lipids. The effect on muscle mass was okay and in about 3 months I had gained 3.4kg of lean mass and 0.3kg of fat (according to a DEXA scan) – no change in training or diet. However, I stopped due to its adverse effects on my endogenous sex hormones and because oxandrolone seemed to dehydrate me.
Interestingly, even such a low dose of oxandrolone caused me to shed about 1kg of water weight, which may have been due to a decrease in estradiol (or estradiol signaling). I am quite lean (usually between 9-11% body fat) and even small changes in water or muscle lead to noticeable effects.
In fact, the combination of the slightly increased muscle mass and the slight loss of total body water caused me to look visibly more “cut” and bigger in a way that others were commenting on it, even though the scale was hardly affected.
A friend of mine who tried it said that his libido decreased and his voice turned to shit, presumably because he lost a bunch of water weight leading to reduced vocal cord mass affecting vibratory capacity.
How it works
Oxandrolone is an androgen acting on the androgen receptor. It is a DHT-derivative and therefore does not interact with 5-alpha-reductase or aromatase. It is also devoid of progesterone effects.
Oxandrolone has about six times the anabolic potency of testosterone (anabolic-androgenic ratio of about 1:6 or so). Unlike DHT, it is not a substrate of 3α-hydroxysteroid dehydrogenase and can therefore exert its anabolic effects in skeletal muscle. DHT, which is inactivated in skeletal muscle, is poorly active in skeletal muscle despite greater androgen receptor binding.

If I ever want to turn to anabolics, I would use a normal TRT protocol (e.g., 75mg testosterone cypionate per week split into daily injections + about 50 IU of HCG daily) in conjunction with a low dose of injectable methenolone (Primobolan) or a low dose of sublingual oxandrolone (Anavar), two DHT-derivative steroids with favorable anabolic-androgenic ratios and devoid of unwanted estrogenic or progesteronergic effects.
Teriparatide
There is an unknown but powerful agent that has the potential to give every person great bone health. This agent is teriparatide.
Teriparatide is a synthetic analog of parathyroid hormone (PTH), which is important for regulating plasma calcium levels and bone metabolism. Continuously high levels of PTH are catabolic to bone but intermittently high levels (e.g., when given once daily), have potent osteoanabolic effects. In fact, PTH-analogs are the most potent bone-building molecules currently available.
Given that bone mass degenerates with age, often leading to fractures that eventually result in inactivity and sarcopenia, it makes sense to boost bone mass using teriparatide at least once after a certain age (e.g., 50 years).
Obviously, with very few exceptions every women should be on HRT after menopause (topic for another day). However, this is often not enough.
People shrink with age and their spine is subject to microfractures, causing back pain and functional impairment. Furthermore, after a femoral neck fracture (which is by no means rare), all-cause mortality rises by 500-1000% (even higher in frail individuals with comorbidities) during the first year and often remains close to double for the rest of the person’s life. One in three women and one in five men will have a hip fracture after age 50. While not as bad as femoral neck fractures, they are still associated with a 40-50% increase in mortality over 5 years.
Furthermore, given that mobility will be somewhat impaired forever after fracture (as old people have a hard time regaining muscles) this leads to a huge impairment in quality of life, for example, a reduction in walks, less social interactions, and a lesser ability to exercise. Which then leads to all sorts of secondary and tertiary consequences.
I worked with a university osteologist before and I asked him what he would do himself if he himself had osteoporosis. His response: 1) Take teriparatide for 2 years. 2) Do a single infusion of zoledronic acid (or oral alendronate for a couple of months) after teriparatide treatment ends to prevent some bone loss as after teriparatide the bone is in a state of increased remodeling resulting in a rapid bone loss upon cessation of teriparatide (only for a few months and by far not enough to make up for the teriparatide gains) – bisphosphonates prevent this state of heightened remodeling/bone loss.
However, this should not be just reserved for osteoporotic folks but can (and in my opinion should!) be done by every person after age 50. If every person did this after hitting age 50 or 55 I am sure that we would slash fracture rate by a decent amount.
I know a couple of people who used it (including myself but to recover more quickly from labral surgery). Other than some lethargy after injection initially (just use it at night!) nobody had any side effects. What are the risks? A tiny uptick in osteosarcoma barely worth mentioning – particularly if people only use it for 2 years. In numbers, the Forteo Patient Registry tracked about 100.000 patients and found only 5 confirmed cases of osteosarcoma which is barely higher than the general population (about 3-4 per million).
Teriparatide is synergistic with weight bearing in the same way that anabolic steroids are synergistic with resistance exercise.
Given access to the drug, this is how one can get a decent uptick in bone mass for decades to come. There is preliminary research that teriparatide also helps a little bit with cartilage tissue as it is supposed to have chondroregenerative effects – particularly peri-injury.
Pregnenolone
Despite what some people claim, I have not noticed anything from pregnenolone, and neither did it affect any of my hormones.
How it works
Pregnenolone is a steroid hormone precursor high upstream in the steroidogenesis pathway (top far left).
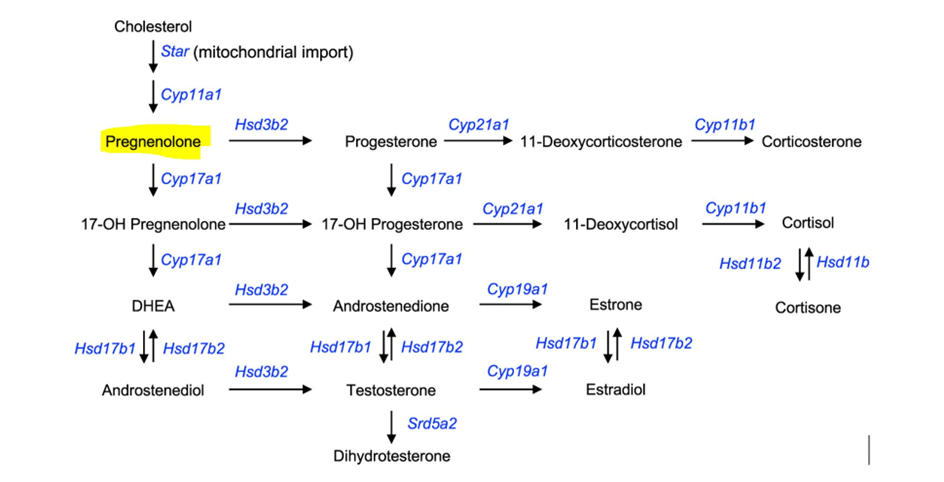
In theory, adding pregnenolone would increase levels of other hormones because of the increased availability of building blocks for steroidogenesis. However, because of various inhibitory feedback mechanisms, this is often not the case. For me, pregnenolone did not change levels of DHEA, DHT, E2, testosterone, or cortisol in any meaningful way.
Pregnenolone is also the precursor to a bunch of neurosteroids with a wide variety of effects.
Some people claim that pregnenolone increases energy levels and causes insomnia (an increase in cortisol?), increases libido (an increase in DHT, T, E2?), and others claim that it improves their memory (an increase in certain neurosteroids?).
DHEA
I experimented with DHEA to see whether it would affect my total testosterone levels. I measured my testosterone at baseline (730ng/dl) and after about 1 month of 50mg DHEA per day, my total testosterone decreased to about 683ng/dl.
The minor decline in T levels could have been due to DHEA (which disproportionately acts on the liver if taken orally) decreasing SHBG synthesis or simply due to normal laboratory fluctuations. Unfortunately, I have not measured SHBG or estradiol.
Libido and other testosterone-related aspects were unchanged. I also did not feel any different.
How it works
Similar to pregnenolone, DHEA is a precursor to sex steroids (but not other steroids).
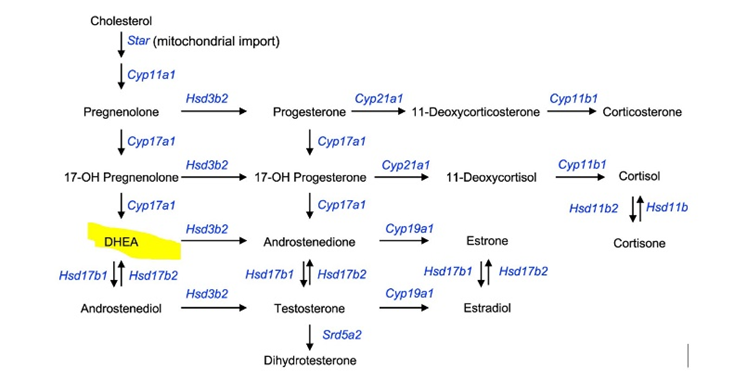
DHEA itself can be converted to DHT, testosterone, and estradiol, either extracellularly or intracellularly. It seems that an increase in sex steroids happens particularly for women or older men but not so much for younger men. Some women report that DHEA increases their sex drive
I personally think it is a good idea for postmenopausal women (or women taking oral contraceptives) to add a low dose of DHEA to partially counteract the loss in androgen levels.
In both genders, DHEA levels decline sharply with age.
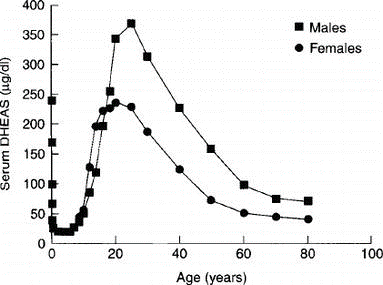
Of note, molecule per molecule, DHEA is the most abundant hormone in the human bloodstream.
GLP-1 analogs
I have experimented with both liraglutide and semaglutide. I talk about my experience with GLP-1 agonists in more detail here.
Disclaimer
The content on this website represents the opinion and personal experience of the author and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without a doctor’s supervision. The content presented is exclusively for informational and entertainment purposes. Never disregard professional medical advice or delay in seeking it because of something you have read on the internet.