
Warning & Disclaimer: Nothing that is presented below is medical advice or a substitute for medical advice. The following represents only what I personally (n=1) would do if I were depressed.

This article has three parts. Part I discusses some general aspects of depression. In part II I discuss a host of interventions other than antidepressants. Part III covers antidepressants.
Part I: Depression
Anecdote time
A couple of years ago, I was in a dark place. I had just finished my biggest exam, and the weeks before were incredibly stressful and brutal. On top of that, my mum was diagnosed with breast cancer and I had just moved out of my apartment.
I felt incredibly lost. I could not think clearly and I started to question myself, the path I was on, and I regretted a number of bad choices I had made. I felt that my friends were not supporting me (though in hindsight they clearly were) and I felt unloved and unlovable.

Although I have not been officially diagnosed, this may have been a major depressive episode. Depression is scary because when I was in the middle of it, I could not imagine there being any hope or any possible way I, or my life, could recover.
I could have been feeling great just a few days ago but once I was at the bottom that did not matter. I wholeheartedly believed that my life was screwed for good and I knew with certainty that it would never get better and there was nothing I could do about it.
Major depression is not just some made-up term for people having a bad day – it is a serious mental state, characterized by a severe imbalance in gene expression and neurotransmitters, which makes the individual emotionally unstable, unable to focus or to think clearly, kills joy, and removes interests (sometimes including one’s own survival).
Even though I had come on and off a number of drugs many times, I now lacked the self-confidence to treat myself with antidepressants out of fear that I would make things worse. After a lot of research and hesitation, I talked to the head of the psychiatry department, and he assured me that vortioxetine was an excellent choice. This reassurance meant the world to me.
Even though I was told to start at 5mg, I started at just 1.25mg because I am a CYP2D6 poor metabolizer (and frankly, because I was quite scared). I could already feel its effect on the first day – and I am quite sure it was not a placebo effect.
The neurobiochemical alterations brought about by vortioxetine changed my outlook on life and the world shockingly quickly. I forgot how bad it was within just a period of a few days, and after a few weeks, I had gotten used to my new state, and my “old” state seemed like a distant dream. This seems to be a common theme.
Six months later, I felt that vortioxetine had mostly done its job and I was again in a good place (mentally, physically, life circumstances). After 3 more months, I tapered off.
This starkly reminded me again of something I had known for a long time: I am a biological creature, and my emotions, thoughts, outlooks, and thinking patterns are at the mercy of my neurobiochemistry and its changes.
The mind is what the brain does.
But why do people get depressed?
The following words are not mine, but from a fugitive psychiatrist who once upon a time wrote a blog, which has unfortunately been taken offline.
“Life is being lost in the desert. It’s just one endless, sweaty, meandering walk over a bunch of empty sand dunes, generally by yourself, maybe with a camel if you’re lucky. Depression is when you temporarily lose the ability to put one foot in front of the other, when you can no longer see in front of you because of the heat and sweat and sand in your eyes.

Suppose your spouse divorces you and takes your children. You eventually slip into a genuine DSM-5 depressive episode – we’ll say four weeks of feeling very sad most of the time, having no interest in life, difficulty sleeping, loss of appetite, difficulty focusing and making decisions, and thoughts of hopelessness and suicide.
If I perform a dexamethasone suppression test, I might find evidence of HPA axis hyperactivity. I might conclude that the HPA axis is somehow involved in the pathophysiology of depressive symptoms. But if I conclude that your depression was simply caused by HPA axis hyperactivity then I’m an idiot.
So, why do people get depressed? You might as well ask me why people fall in love. Any answer to both questions would involve some speculation about neurotransmitters and hormones, environmental triggers, early childhood experiences, genetics, and evolution, all wrapped within a culturally determined epistemological framework.
To go from being not depressed to depressed inevitably involves changes in your brain. Everything you think, feel, and do is mediated by neural activity, so changes in your typical patterns of thinking, feeling, and doing have to involve changes in your brain.
However, to say that these hypothetical neural changes caused you to become depressed in and of themselves would be a bit of a stretch. They may have mediated the transition from being not depressed to depressed, and in that sense were a necessary step in a chain of events.
But they were probably not the ultimate or primordial cause, simply because the majority of depressive episodes occur in response to obvious environmental triggers. The same could be said of falling in love, which as far as I can tell is equality indicative of brain pathology. (…)
Imagine you’re standing on top of a big hill. At the very top of the hill, things are alright, you’re feeling reasonably content and happy, or at least like your normal self. As you walk down the hill you slowly start to feel a bit more depressed: sad, hopeless, exhausted, pessimistic, disinterested in life, whatever being “depressed” feels like to you. Then all of a sudden there’s a sharp drop, and you tumble to the bottom of the hill. Now you’re depressed.

There are things in life that push people towards becoming depressed: chronic stress and anxiety, trauma, loss, physical illness, social isolation. You can think of these things as a wind, from the East no doubt, pushing you down the hill.
This is an important thing to remember: everybody has a hill. The shape of the hill, or the threshold for becoming depressed, is influenced by a lot of things, including genetics, temperament, exposure to certain substances, childhood trauma/adversity, shitty parents, and other fun life experiences.
Some people’s hills are really steep, it doesn’t take much of a wind to send them tumbling down. Other people have hills with long, flat tops; it takes a serious amount of wind to get them to the bottom. Some people have a hill that’s really tall, so they’re normally pretty happy and upbeat when they’re at the top, but it may still be a steep hill with not much room on top. Some people have a short hill, and even though they may never get blown to the bottom, they’re still normally kind of gloomy, low-energy, low-excitement.
Antidepressants are one of the many tools people can use to make the climb a bit easier. They’re like crampons, but with more side effects.”
Depression
The term depression was derived from the Latin verb “deprimere”, which literally means “to press down”. Depression is defined as “a downward deviation from baseline”, for example, neurobiological depression, economic depression, or geological depression.

For example, if a generally happy and cheerful person (top of the hill) experiences depression and their happiness and cheerfulness are now gone (bottom of the hill), their “baseline state” is depressed in the most literal sense of the word.
However, “Some people have a short hill, and even though they may never get blown to the bottom, they’re still normally kind of gloomy, low-energy, low-excitement.” Many people who think they are depressed (”I have been depressed my entire life and I never really enjoy anything.”) are not really “depressed” (from a neurobiological perspective) because they are always this way.
For many people, dysthymia (constant low-grade depression) is their natural state, and they are always unhappy, dissatisfied, self-loathing, and have little energy, joy, or motivation. Unfortunately, the term “depression” is used interchangeably to describe both the disorder (characterized by a marked downward deviation from baseline) as well as persistent dysthymia (characterized by having an awful baseline state).
In this article, I describe how I personally would go about treating depression, whether the “neurobiological” type or the ”I-have-been-depressed-my-entire-life-and-I-never-really-enjoy-anything”-type.
My depression is not your depression
As hinted at already, one thing that makes depression so frustrating is that “depression” is such a broad concept and fuzzily defined. One person’s symptoms include no satisfaction from listening to music or time spent with friends (anhedonia), but they report having a decent sex drive and no issue concentrating at work. Another person might feel constant sadness. Another person may feel at the bottom of the social hierarchy due to not having money, status, or looks. Another person always feels drained and lethargic. Another person has extremely poor self-worth and morbid thoughts. Another person simply feels “hollow”.
I am prone to anhedonic depression. Even in my “depressed” periods, I am highly driven to do stuff. I write articles, work, go to the gym, meet friends, and date. However, inside, there is emptiness. I feel little to no anxiety but also little to no joy (anhedonia). Thus far, a single injection of ketamine (discussed later) was always sufficient to get me out of it and my emotional tone is back on. Fortunately, these episodes have been getting rarer.
There are a large number of similar permutations with a large number of various symptoms felt by millions of people, some of whom ask their doctors for help, only to be given a single-word diagnosis: “depression.”
Obviously, in the vast majority of cases, depression is not “isolated” in the brain but rather intricately related to a certain life situation, such as the loss of a loved one, addiction, loneliness, untreatable illness, etc.
Unfortunately, most of the people get prescribed the same treatments…
I discuss different kinds of depression here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Part II: Antidepressants
In the case of depressive episodes (but not in the case of persistent dysthymia), many times people get better on their own. Meta-analyses suggest that about 30% of people remit spontaneously in about 6 months and a little over 50% after a year.
This however, is not to say that antidepressants aren´t useful or could not accelerate things, particularly if the person has been chronically dysthymic or sub-depressed for a long time as chronic, long-standing issues are less likely to get better on their own compared to acute, short-lived issues.
There are all kinds of ways to cope: medication, therapy, alcohol, drugs, sex, gambling, work addiction, withdrawal, etc. Medication isn’t the worst one by far.
As mentioned already, the term “depression” has taken on multiple meanings and what most lay people mean by “depression” (a number of non-specific states of persistent unhappiness, life satisfaction, low self-esteem, self-loathing, and low excitement) may not always correspond to what doctors mean by “depression” (a number of different kinds of neurological processes that are associated with a marked downward deviation from an individual’s baseline).

Clinical trials for antidepressants enroll people with MDD who are currently in depressive episodes, not people who are chronically unhappy and hate their lives. However, even though antidepressants have only been scientifically assessed for their efficacy in treating the former type, they can still be moderately effective in addressing the latter type by helping with emotional regulation, pessimistic thinking patterns, and most importantly, improving an individual’s life situation.
I discuss this in more detail in The Power of Neurobiochemistry.
Should I take an antidepressant?
The answer to this question is obviously individual. Antidepressants have both upsides and downsides.
The downsides and side effects of antidepressants need to be weighed against the downsides and side effects of depression. Not treating depression adequately may have a number of severe 2nd and 3rd-order consequences, such as potentially falling out with family or friends, getting laid off from work, or engaging in bad lifestyle behaviors such as forgoing exercise, bad sleep, substance abuse, or having a crappy diet, all of which have their own long-term sequelae. However, for many people antidepressants are not necessarily needed. Nonetheless, they are useful tools.
Different kinds of antidepressants
There are a variety of different classes of antidepressants, including SSRIs, SNRIs, tricyclics (TCAs), NDRIs, MAO-inhibitors, and a variety of atypical antidepressants that are hard to classify (e.g., trazodone, mirtazapine, agomelatine, ketamine).
Unfortunately, many doctors tend to give out the same kind of antidepressant to anyone. Most depressed people are likely to be started on an SSRI – regardless of a patient’s symptomatology.
However, whether a doctor chooses e.g., escitalopram (the prototypical serotonin reuptake inhibitor) vs. bupropion (a noradrenaline and dopamine reuptake inhibitor) makes a fairly large difference in how the patient feels and performs for the time the patient is on the drug (even though statistical equivalence may tempt doctors to believe otherwise).
The choice of antidepressant will eventually have a number of potentially far-reaching 2nd and 3rd-order consequences on many domains of a patient’s life ranging from work, relationships, sleep, lifestyle choices, and thinking patterns.

Different kinds of depression are best treated with different drugs. Some researchers speculate that anxious depression is in part characterized by a relative deficiency of serotonin signaling (very simplistically speaking), while anergic or “atypical” depression is characterized by a relative deficiency of catecholamines, especially dopamine. Whether this is true or not is controversial.
Nonetheless, it seems that anxious individuals with poor self-worth seem to fare reasonably well with SSRIs. SSRIs are particularly effective if the individual has symptoms of anxiety or OCD, which may be causally related to the development of depression.
Conversely, for people with lethargy, anhedonia, and a lack of motivation as their main depressive symptoms, SSRIs often exacerbate the issue, as excess serotonin is thought to reduce dopamine signaling by serotonergic modulation of catecholaminergic midbrain neurons. In my opinion, anergic (“atypical”) individuals fare better with DNRIs or MAO inhibitors.
Sometimes, depression is due to ADHD, which is treated differently altogether. I share my thoughts on the treatment of ADHD in more detail here.
So, what kind of antidepressant would I choose?
If I were depressed, my first choice would be bupropion, sertraline, or vortioxetine, as all of these are, in my opinion, great general-purpose antidepressants with reasonable side effect profiles. Escitalopram is also a reasonable choice, though has a higher incidence of emotional blunting. If I were more anxious than depressed, I would choose one of the SSRIs and if I were more depressed than anxious, I would choose bupropion. Combining escitalopram + bupropion, preferrably in low doses, is also a decent strategy and is commonly done in practice.
My personal favorite is moclobemide, though for a variety of reasons I believe that moclobemide is a suboptimal first-line antidepressant.
Recently, more and more psychiatrists started using modafinil to treat depression, sometimes alone and sometimes as an adjunct to other antidepressants. Modafinil is the only pure dopamine reuptake inhibitor currently in clinical use. In my opinion, modafinil is a safe and underrated antidepressant and its effectiveness confirms the importance of dopamine for depression. I discuss my experience with modafinil in more detail here.
Very simplistically speaking, dopamine has to do with motivation, noradrenaline with alertness, and serotonin with calmness. In reality, things are more nuanced and complex and I discuss the basics of neurotransmitters here: A Brief Introduction to Neurotransmitters (and How to Modulate Them)

A brief background on the drugs mentioned above:
- Buproprion is a classified as a dopamnie-noradrenaline reuptake inhibitor (DNRI). In reality, it is much stronger on the noradrenaline front than on the dopamine front. On 300mg of the drug (the standard dose), noradrenaline transporter (NET) occupancy is roughly 50-60% and dopamine transporter (DAT) occupancy is only about 20% (vs. e.g., 60% for 200mg of modafinil). I discuss bupropion in more detail here.
- Sertraline is an SSRI, meaning it blocks the serotonin transporter, which causes serotonin to accumulate in the synaptic cleft leading to longer serotonin signaling. Next to the serotonin transporter (SERT), sertraline has an appreciable affinity for the dopamine transporter and is, therefore, an often-used “all-rounder”. Unfortunately, it has a high incidence of sexual dysfunction, among the highest of all SSRIs. I share my thoughts on SSRIs in more detail here.
- Escitalopram, the s-enantiomer of citalopram, is the “prototypical” SSRI. It is the cleanest because it is the most SERT-selective. Next to binding to the typical SSRI site, it also binds to an allosteric site which decreases SERT performance, and therefore it may increase serotonin levels more than other SSRIs. It has a comparatively low incidence of sexual dysfunction.
- Vortioxetine is also an SSRI, but a somewhat atypical one. Vortioxetine is an SSRI plus a serotonin receptor modulator, modulating 5HT3, 5HT1A, and 5HT7 receptors. It is the newest SSRI brought to market. Even though people’s reactions to drugs differ, the unique properties of vortioxetine make it, in my opinion, a decent choice as a first-line antidepressant. It has a lesser incidence of emotional bluting and a lesser incidence of sexual dysfunction, which are the most bothersome SSRI side effects. I discuss vortioxetine in more detail here.
- Moclobemide is a reversible inhibitor of monoamine oxidase A. MAO-A metabolizes all three major monoamines, so MAO-A inhibitors elevate serotonin (strongest), noradrenaline (strong), and dopamine (weakest). Moclobemide is a poorly known all-rounder. It boosts energy levels, mood, sleep, and hormones. On the therapeutic side, it helps with anxiety, obsessive-compulsive symptoms, depression, a lack of energy, and ADHD symptoms. All while not blunting emotions, worsening libido, or dysregulating appetite in a way many other antidepressant drugs do. However, moclobemide comes with dangerous drug interactions. And some people poorly respond to it for some reason. I discuss mocolobemide in more detail here.
- Modafinil is a weak inhibitor of the dopamine transporter (DAT), which presumably accounts for the majority of its effects. In fact, modafinil is the only pure dopamine reuptake inhibitor in clinical use (since amineptine was taken off the market in most countries). At a dose of 100-200mg modafinil, the DAT occupancy is about 50-60%. What is poorly known to most doctors is that modafinil is a great stand-alone antidepressant (and also a great augmentation agent) confirming the importance of dopamine in depression. I discuss modafinil in more detail here.
Antipsychotics and mood stabilizers are frequently prescribed add-on medications for the treatment of depression. Their use should be reserved for specialists and I briefly discuss some of them here. In my opinion, overprescribing antipsychotics for the garden weed type of depression, which is unfortunately often done, amounts to malpractice.
The triple-reuptake inhibitors ansofaxine and dasotraline are currently in clinical trials and both of these molecules seem to hold some potential, particularly as they target all three major monoamines. I discuss these and a couple of other potentially novel antidepressants here: Noteworthy Molecules Stuck in Pharmaceutical Pipelines.
We are all different
I have experimented with many different molecules and I found that my response to a certain neuropharmaceutical is a very individual matter, and it is awfully hard to predict whether I respond well to something or not, regardless of what doctors, the medical literature, or anecdotal online reports make me believe. The only conclusive way to figure out how I respond to something is to try it.

Side effects
The most dreaded antidepressant side effects are emotional numbing, weight gain, and sexual dysfunction, all of which are common to SSRIs (more to some than others), particularly at higher doses. Unlike most of the annoying side effects (such as anxiety, diarrhea, insomnia, and dry mouth) these usually do not go away on their own.
Vortioxetine is a little less likely than other SSRIs to cause these side effects, though still well above placebo.

The only common antidepressant that does not have these side effects is bupropion. Moclobemide, agomelatine, nefazodone, reboxetine, and selegiline do not have these either, though they are much less commonly used.
Bupropion deserves a special mention. It is the only frequently prescribed antidepressant that does not cause weight gain, emotional blunting, sedation, or sexual dysfunction – quite the opposite: It tends to improve energy levels, emotional regulation, and sexual function, and it tends to cause weight loss. Furthermore, it helps with ADHD symptoms. Reportedly, it also has a milder withdrawal than other antidepressants.

Unfortunately, given that most people with depression experience some form of anxiety (and most meet diagnostic criteria for an anxiety disorder) bupropion is rarely used as a first-line antidepressant because many doctors think that it worsens anxiety, which is not actually the case and contrary to popular belief, there is convincing evidence to support the notion that bupropion and SSRIs are equally effective for treating “anxious” depression and bupropion is no more likely to worsen anxiety than SSRIs (other than perhaps during the first few weeks of treatment).
Because this dogma still prevails among doctors (including most psychiatrists), a lot of patients have lost their sex lives.
I discuss bupropion in more detail here.
Starting dose
Contrary to medical advice, I would start an antidepressant at only ¼ to ½ of the lowest prescribed dose, particularly if I were worried about side effects and then slowly increase from there.
For example, when I started bupropion or vortioxetine, I quartered the tablets and started with only 25% of the lowest recommended starting dose (37.5mg for bupropion and 1.25mg for vortioxetine). I then increased the dose by one-quarter every couple of days. This way, for me, the initiation was smooth and quite devoid of unnecessary side effects.
I have recommended this strategy many times to others, both to friends as well as patients, and for most people, this is presumably the most rational way to go about things.

Target dose
Antidepressants have a decent efficacy if they are dosed at very low doses – which also reduces side effect burden – and in my opinion, antidepressants are usually dosed much higher than they need to be, especially for cases of light uncomplicated depression. According to clinical data, the proportion of responders (remitters) at high doses is not impressively larger than at lower doses.
In my experience and the experience of some of my friends, subtherapeutic doses (doses lower than the lowest prescribed dose) have decent benefits, and more importantly, much fewer side effects. For example, a good friend of mine manages his seasonal affective disorder effectively with only 2.5mg of escitalopram (half of the lowest prescribed dose). He even finds 1.25mg quite effective – and more importantly, mostly devoid of side effects.
When my mother went through chemotherapy, she was gripped by fear and sadness and got depressed. I gave her some escitalopram. 2.5mg was all that she needed. Quite soon after, parts of her “old” personality came back and she started to laugh again. Also, her friends noticed how her voice had gotten stronger. Even though 2.5mg of escitalopram is a “placebo-dose” to most psychiatrists.
Unfortunately, many doctors seem to rapidly increase to a high dose, which not only is associated with increased side effects but maxing out the dose also prevents them from increasing the dose in the future when they need to (and then, the only remaining options are polypharmacy or starting from scratch).
In summary, lower doses are decently effective, have fewer adverse effects, and allow for increasing the dose when one needs to.
Timing
Most antidepressants are taken once a day. They can be taken at any time, given that the time of the day is roughly the same between days because otherwise, plasma levels (and therefore symptoms) may fluctuate. For example, if a medication makes me sleepy, taking it at night makes obviously more sense than taking it in the morning.
How long should I take an antidepressant?
It surely depends on whether I had a depressive episode (biological depression) or whether I was chronically dysthymic (“suffering”).
In case of a depressive episode, it is usually recommended to take antidepressants for at least six months after remission, though according to my reading of the available data, relapse rates do not seem to be much different than taking antidepressants for around four months after remission.
In case of chronic dysthymia or unhappiness, I would take antidepressants for at least as long as the necessary life changes have been made.
An important point of taking antidepressants is to help with making real-life-changes
A psychiatrist once told me that the people who don’t want to do anything except take pills are usually the patients who have been on a dozen different medications, and nothing ever seems to help. With very few exceptions, no antidepressant in the world will be capable of completely undoing years of pessimistic thinking, self-loathing, disinterest in life, absence of high-quality relationships, etc.
Antidepressants are intended to reverse depression-induced neurobiochemical changes, improve emotional regulation, and help with pessimistic thinking patterns. However, one of the major but often neglected points of taking medication is not exclusively to make the “suffering” go away, but also to help people to improve their life circumstances. Unfortunately, the “number of important life changes made” is a hard-to-measure secondary endpoint.

While medication may help to rekindle some interest in life, if I do not actually get going and do something, medication may only help me temporarily to tolerate a life that I should not tolerate. In other words, antidepressants may help to kickstart the motor, but if the car does not go anywhere, it won’t matter that much.
In my opinion and experience, dopamine enhancement is particularly helpful for this because dopamine not only “feels good” but also motivates me to take action. Unfortunately, dopamine is unfairly neglected by most current antidepressant regimens. I discuss this in more detail here: The Brutal Neglect of Dopamine
Can the scientific literature help me decide what kind of antidepressant I should choose?
Drug trials only evaluate the efficacy of antidepressants in major depressive episodes (MDD) and not in the chronic suffering-dysthymic-“I hate my life” type of depression, one of which is a neurobiological disorder and the other is (usually) not. However, many people with depression are of the second type.
Furthermore, the medical evidence-generation process has many issues.
- Firstly, most of the trials are industry-sponsored and contain highly selective samples. It is thought that only 10-20% of psychiatric outpatients (and about 0% of psychiatric inpatients) would meet the selection criteria.
- Secondly, the data is often tortured in a way that amounts to faking. Usually, relative ratios are given and improvement in absolute terms is often small.
- Thirdly, statistical significance does not mean a drug works well, or at all. In a trial with enough patients, any difference will be statistically significant.
Because of these mismatches between clinical trials and real life, a billion meta-analyses reanalyzing the same kind of primary data cannot tell me if a specific antidepressant is effective at my individual level.
For example, in most RCTs or meta-analyses it does not make a statistically significant difference whether a patient is prescribed the DNRI bupropion or the SSRI escitalopram. Usually, in both groups around 40% or so of patients remit within 8 weeks, and from a numerical perspective it would seem that these two drugs were equal.
However, from a first-person perspective, these two drugs feel vastly different (as they also work on completely different neurotransmitter systems). Because this qualitative difference is hardly captured in the scientific literature (other than in side effect profiles), in my opinion, first-hand accounts by real people of what it is like to take a certain drug are perhaps as, if not more, valuable than PubMed literature.
Furthermore, much of the published literature on a subject is often not applicable to real-life people (probably because of the invasion of academic medicine by the industry). For example, “large-scale clinical studies have not found evidence of tolerance with modafinil at therapeutic doses even with prolonged use” or “eszopiclone administered for a period of up to 12 months was associated with a sustained beneficial effect on sleep induction and maintenance, with no occurrence of tolerance”, which is flying in the face of every real person who takes these drugs.
I personally find it more helpful to read a large number of different real-life experiences on Reddit than getting hung up on statistical odds ratios.

Combination regimens?
Even though all of the monoamine and non-monoamine neurotransmitter systems are interconnected and changes in one system produce downstream changes in the others, one major drawback of using antidepressant monotherapy (i.e., single-drug regimen) is that the relative activities of the individual neurotransmitters cannot be “customized”.
Combining distinct types of antidepressants that target different neurotransmitter systems allows for personalized adjustments of neurotransmitter levels, just as a graphic equalizer allows for the customization of audio frequencies.

With creative psychopharmacology, I could, in theory as well as in practice, adjust the activities of individual neurotransmitters according to my needs, tolerance, and preferences.
For example, instead of relying on duloxetine (an SNRI with a SERT:NET ratio of 4:1), I could combine an individualized dose of escitalopram, a pure SSRI, with an individualized dose of reboxetine, a pure NRI.
Or I could create a customized triple-reuptake inhibitor (serotonin, dopamine, noradrenaline) by combining individualized doses of escitalopram, atomoxetine, and modafinil. However, such cosmetic fine-tuning is rarely done by conventional psychiatrists.
Two friends have had great results with the lowest prescribed dose of bupropion (targeting noradrenaline and to a lesser extent dopamine) plus the lowest prescribed dose of vortioxetine (targeting serotonin). (Note: Vortioxetine is metabolized by CYP2D6, which bupropion blocks, and therefore vortioxetine plasma levels may be higher than expected.)
Frequently employed combination regimens are mirtazapine + venlafaxine (“California Rocket Fuel”) and bupropion + escitalopram. I personally liked the combination of low-dose moclobemide + low-dose rasagiline, though I have not used it to treat depression but rather to “get more out of life” (though, I have stopped taking it for a number of reasons discussed here).

As always, the ideal drug regimen is best found by cautious empirical self-investigation.
“Nuclear” options for treatment-resistant cases
The label “treatment-resistant depression” is poorly chosen. If I were diagnosed with it, it would cultivate a sense of despair and hopelessness and it would make me believe that I have “incurable” depression. More often than not, the diagnosis is given due to misdiagnosis (e.g., ADHD), incompetent psychopharmacology (e.g., trying a patient on an SNRI after he already failed two SSRIs), or a patient’s unwillingness to do anything other than take medication.
Nonetheless, if none of the garden-variety antidepressants mentioned above would work, and if I was suspecting that my depression had a large biological component to it, I would probably consider turning to heavier guns such as ketamine, irreversible MAO inhibitors, weak opioids, or dopamine modulators because I feel that the only life I can be sure of having is too short and precious to feel awful all of the time.
Ketamine
Were it not for the (potential) neurotoxicity, ketamine would be the near-perfect antidepressant. Unlike other antidepressants on the market, it works very rapidly (within 24 hours), it does not “distort” monoamine balances, has no side effects (other than temporary dissociation and increases in blood pressure during the ketamine experience itself), few risks if used at adequate doses (e.g., bladder toxicity is dose dependent) and only needs to be taken once every or every other week, sometimes even only once every couple of months. Furthermore, ketamine seems to work for many people for whom nothing else works.
Ketamine is especially useful for deep “biological” kinds of depression, but much less useful for the “suffering”-type of depression.
The major downside is potential neurotoxicity. Whereas ketamine increases the generation of new spines (spinogenesis) and synapses (synaptogenesis), it may irreversibly kill off neurons. Newly formed spines and synapses can and will regress, however, dead neurons will never undie. It is hard to say whether this already occurs at subanaesthetic doses taken occasionally but microscopic brain damage is plausible at even low doses.
I discuss ketamine, and my experience with it, in more detail here.

Irreversible MAO inhibitors
Some people experience spectacular remission of depression, apathy, anhedonia, and lethargy on irreversible MAO inhibition when nothing else has worked. Phenelzine is more calming while tranylcypromine (an amphetamine derivative) is more activating. Irreversible MAO-inhibitors are perhaps the strongest antidepressants on the market and there are many reports of people being stably remitted for decades on these drugs. However, irreversible MAO inhibitors come with considerable risks (e.g., drug and food interactions that can be really dangerous) and side effects (mostly low blood pressure issues).
Irreversible MAO inhibitors are discussed here.
Weak opioids
While dopamine mediates “wanting”, mu-opioids mediate “liking”. I discuss opioids in more detail in my article on tianeptine.
Even though opioids are uniquely effective at banishing depression, the opioid system has thus far been left mostly (and understandably) untouched – much more so than the dopaminergic system, which is the other neglected transmitter system pertaining to well-being and not just the elimination of misery.
Using opioids for the treatment of depression is a legal and ethical minefield since they are addictive and hard to withdraw from. Nonetheless, weak opioids such as tianeptine (a weak mu-receptor agonist), buprenorphine (a mu-partial agonist and a kappa-antagonist), or tramadol (a weak mu-receptor agonist, and an SNRI) sometimes have great therapeutic effects when nothing else had worked.

At least for a short period of time (until desensitization & counterregulation set in), opioids are incredibly effective at treating depression.
Opioids are discussed here.
Dopamine modulators
Pramipexole, a partial agonist at a variety of dopamine receptors (D2, D3, D4), particularly the D3 receptor, deserves special mention. Some people experience significant relief, though others become slaves to their vices (e.g., drugs, food, porn, etc.). Cabergoline is an alternative that also works for some people.
Low doses of cariprazine, amisulpride, and aripiprazole are also sometimes useful. At low doses, they block D3 autoceptors, which disinhibits dopamine release, thus elevating dopaminergic tone in a similar way pitolisant elevates histamine levels by blocking H3.
I discuss some dopamine modulators in more detail here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Psychedelics
A friend (and doctor), who has been on every antidepressant under the sun says that the only thing that truly cures his depression is psylocibin. He takes 2g once per week. Reportedly, he feels little to no “trippy” effects but it somehow cures his depression.
It took a couple of weeks for everything to settle down but he has now been depression-free for about 10 months, after struggling with depression for roughly 30 years, including multiple hospitalizations and one suicide attempt. He believes that the trip itself is much less important than the effect of psychedelics on neuroplasticity, something that recent literature seems to bear out as well.
Lately, a lot of hype has been forming around psychedelics and there is now a vast amount of decent literature hinting at their effectiveness in depression. I have heard from a lot of people that psychedelics really helped them.
On a molecular level, some of the antidepressant effects of psychedelics are somewhat similar to ketamine. A short 15 min to 1 h stimulation of cultured cortical neurons with LSD leads to neuronal growth that persists long after the compounds have been removed from the culture media. Moreover, after psilocybin administration, a higher density of dendritic spines is observed in the mPFC of the mouse for at least 1 month.
Both ketamine and psychedelics mediate an increase in both structural as well as functional plasticity (e.g., neuritogenesis, spinogenesis) that presumably follows similar molecular mechanisms (e.g., activation of TrkB and mTOR), both in vitro as well as in vivo. For both compounds, cotreatment with rapamycin reduces their effects (at least in vitro – whereas in vivo effects are more complex and rapamycin potentially prolongs the antidepressant effects).
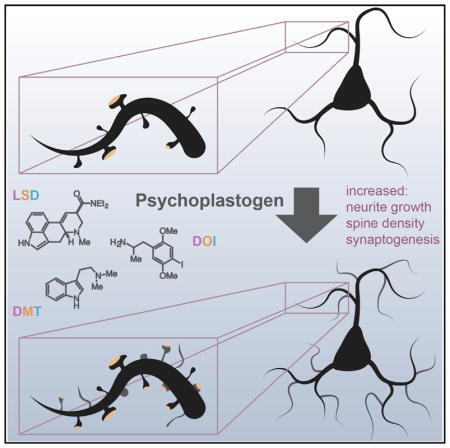
The psychedelic-induced increase in neuroplasticity can also be abolished with ketanserine, a high-affinity 5HT2A-antagonist, indicating that psychedelics mediate their effects on neuroplasticity through the 5HT2A-receptor and not some other obscure target.
In addition to the 5HT2A-receptor-mediated changes in neuroplasticity, there is a huge increase in neocortical activity and neurons of different cortical areas are more connected compared to normal waking life. This means that areas that normally do not communicate much, suddenly do communicate a lot.
Because a mammalian neocortex adapts depending on how it is used, these rarely used “random” connections are strengthened (”use it or lose it”), and new non-ordinary memories are formed. This results in the growth of hippocampal neurons as well as trophic adaptations of synapses & dendrites in a similar (but more potent) way than environmental enrichment (e.g., traveling).
In this sense, psychedelics are basically massive environmental enrichment “in a pill” and are potentially capable of keeping a brain in a more rejuvenated state.
Moreover, psychedelics also have powerful perceptual effects (”a year´s worth of psychotherapy in one afternoon) and in the same way a traumatizing experience (e.g., loss of a loved one, romantic rejection) can trigger neurobiochemical depression, so can a “winning” experience (e.g., finding love, major life success, meaning-giving psychedelic experience) have top-down effects on depression. Furthermore, they help with getting some “deathbed clarity” before deathbed happens so people can actually do something about it. And not to be neglected, psychedelics may help people with feeling more connected to others and/or with finding purpose in life.
Which of these effects is most important (the top-down vs. the bottom-up effect)? The answer is currently unknown but I speculate that it probably depends on the person.
However, I would approach psychedelics with great caution. I discuss psychedelics, the science, and the non-trivial risks in more detail here.
Case reports
Humans are complex and we are all different. I discuss a couple of case reports in more detail here.
Non-conventional “antidepressants”
Hormones
Hormones are deeply connected to nervous system function, having potent effects on energy levels, mood, and well-being. Deficiencies of major hormones can cause states resembling depression. Hormones are very influential on neurotransmitter systems. Moreover, they affect the expression of hundreds of genes, the most powerful layer of intervention.
Hypogonadism (“lowT” for males; females on birth control or females with low estrogen) often causes a state of low excitement, “mehness”, and dysthymia. An aquaintance who has been chronically depressed for his whole life claims that the only time when he felt well was in the 2 years he was on 250mg of testosterone (which is far higher than a replacement dose). I personally also feel considerably better since starting my TRT lite regimen. Using testosterone as an antidepressant has become quite popular lately. High doses of testosterone can cause hypomania (“feeling better than well”), presumably because of its effects on dopamine levels.
Similarly, hypothyroidism is highly associated with depression, and T3 is a fantastic antidepressant. In the past, when I have experimented with thyroid hormones, I always felt a boost in energy and mood for a few weeks to months after starting thyroid hormones.
Hypoleptinemia (due to having a lower body fat than one should have) is also independently associated with a depression-like state. My times of anhedonic depression are correlated with times my body fat is very low. Leptin administration is highly effective (and likely causal) at reversing it.
Low cortisol levels can cause fatigue-like depression and high cortisol levels can cause a restless kind of depression.
I discuss the power of hormones in more detail here: The Life-changing Power of Hormones
I discuss these hormones in more detail here:
NSI-189
NSI-189 is a molecule that stimulates neurogenesis in the hippocampus and perhaps other sites. Many people find it quite effective for increasing emotional tone. For me personally, it gives me very vivid dreams, increases my libido, and makes me feel more deeply. I discuss my experience with NSI-189 in more detail here.
Most of the NSI-189 available on the black market is presumably bunk and proper NSI-189 can probably only be purchased with a medical/research licence. Thus the major downside is that proper NSI-189 (pharmaceutical grade) is very hard to get hold of.
NSI-189 has been renamed Alto-100.
Metabolic regulators
Some people report antidepressant and anti-addiction effects from taking GLP-1 agonists. Furthermore, GLP-1 agonists cause weight loss and improve looks, metabolic health, and low-level inflammation. GLP-1 agonists are discussed in more detail here.

I discuss other metabolic drugs, such as metformin, SGLT-2 inhibitors, rapamycin, and acarbose in more detail here: Metabolic Drugs – And My Experience With Them.
For some people, GLP-1 agonists can cause anhedonia due to their effect on the dopamine system.

Anti-inflammatory agents
Certain kinds of depression are due to immune dysregulation (“sickness behavior”) and there is evidence that reducing inflammation (e.g., with COX-inhibiting agents) helps with depression.
In fact, certain subtypes of depression may be mistaken for prolonged “sickness behavior”, which is a homeostatic decline in energy levels, mood, self-confidence, and sociability that arises with infection or other inflammatory states.
Indeed, many of the genes associated with depression are involved in inflammation and immune regulation and when even “normal” people get sick, or right before an autoimmune attack, they often feel “depressed”. Celecoxib, a selective COX-2 inhibitor, has decent data in depression in individuals with elevated levels of CRP).
I discuss this in more detail here (Ibuprofen) and here (Low-dose Naltrexone).

Gut health
Some people report improvement in mental health by improving gut health. One friend improved his “meh-ness” by taking a short course of rifaximin, a gut-targeted antibiotic, aiming to “reset” his microbiome.

I share my thoughts on the gut microbiome, and some practical stuff, in more detail here.
Supplements
Regardless of whether I was depressed or not, I would take a couple of supplements, including vitamin D, omega-3 fatty acids (there seems to be a correlation between fish consumption and depression), and magnesium, all of which may have beneficial effects on depressive symptoms, though presumably, the effect sizes are not very large.
L-methyl-folate and N-acetyl cysteine are also promising and, anecdotally, many people respond favorably to them. L-methyl-folate is also frequently used by psychiatrists as an augmentation strategy.
Creatine also has decent evidence behind it and it even seems to be able to induce mania in bipolar people, albeit rarely. An ability to induce a manic switch is an indicator that it is doing something in the nervous system.
I would also do a blood test for ferritin (iron) and vitamin B12, and if necessary, supplement with them. I discuss these supplements in more detail here.

The only supplement I have ever found with true rapid antidepressant effects is S-adenosyl methionine, though unfortunately, it is potentially epigenotoxic.
Some people respond well to 5HTP and L-acetyl-tyrosine. The former is a precursor to serotonin and the latter to catecholamines. According to both anecdotal and experimental data, saffron supplements also seem to have a decent benefit, though I do not know anyone who has tried them.
Some people claim that ashwagandha or rhodiola helped their anxiety and depression. Anecdotally, one friend of mine “cured” her nightmares by taking ashwagandha before bed. Anecdotally, ashwagandha is associated with some emotional blunting, similar to SSRIs (but much weaker in its effect). I discuss my thoughts on herbal supplements in more detail here.
Microdosing lithium
Anecdotally, some people experience some benefits in terms of mood and emotional stability from a microdose of lithium, such as 5mg lithium orotate taken at night (for reference, therapeutic lithium dosages range from 30-200mg of elemental lithium). For others, even a microdose can result in emotional flatness. Adding a microdose of lithium can also improve the response to various antidepressants.
Interestingly, the amount of lithium in the groundwater is correlated with the suicide rate of a particular area.

How exactly lithium works is not fully known, though it seems to boost a variety of neurotransmitters, specifically serotonin. It is hypothesized that lithium inhibits an intracellular kinase named GSK-3, which is involved in a variety of intracellular pathways, and some researchers believe that this is its primary mode of action.
Of note, the longevity physician Peter Attia and “lifestyle guru” Tim Ferris have been taking microdoses of lithium for years, specifically to help with stress and emotional regulation. Anecdotally, a friend of mine said he experiences “profound” mental changes with just 5mg of lithium orotate, particularly in his mood.
“The medication stopped working”
A couple of years ago, I was stressed and anxious. I started meditation. After a couple of weeks, the stress and the anxiety abated, and I felt much better. However, a couple of months later, I was stressed and anxious again (despite meditating): “I guess the meditation stopped working.”
However, this was terrible reasoning. Where would I have been and how would I have felt if I did not meditate every day? Perhaps, I would have been 40% worse and the meditation was still doing something even if I was not aware.
Similarly, for many people, antidepressants eventually “stop working”. However, they alter neurobiochemistry every waking second, and there is no way to tell whether they truly “stopped working” or whether they are simply not working sufficiently.
Long-term personality changes
Some people assume that neuropharmaceutical drugs only treat mental disorders but do not mess with personality. This is bullshit at its best as my personality is nothing more than my pattern of feeling, thinking, and acting, which depends to some extent on my brain wiring and my neurotransmitters, both of which are altered by neuropharmaceuticals.
For example, SSRIs tend to move people toward the middle of the Big Five personality traits, regardless of whether someone is mentally ill or not.

Furthermore, given the brain has evolved to adapt depending on how it is used, taking an antidepressant may entail long-term personality changes that persist after I stop taking the drug. Next to reasoning from neuroscientific first-principles, there are many anecdotal reports to support this.
While this is not necessarily a bad thing, before experimenting with antidepressants, I need to be aware that taking an antidepressant for some amount of time will irreversibly change my brain.
I discuss this in more detail here: Why Does Cocaine Make You Cocky and Why Do Psychedelics Make You Weird?.
Are antidepressants “bad” for the brain?
In short, no, with the exception of ketamine and amphetamines.
There are many independent effects that need to be considered:
- What is the long-term effect of the medication vs. no medication on the brain itself? We know for a fact that depression is quite neurodegenerative itself so even if antidepressants are not optimal for long-term brain health, are they worse than depression? Probably not. However, antidepressants also have direct effects on the brain. For example, SSRIs lead to long-lasting changes in the cytoarchitecture of the amygdala (and many other brain sites). Similarly, other antidepressants also lead to trophic brain changes. Tricyclics are “dumb drugs”, and ketamine and amphetamines are known to be neurotoxic. I discuss the neurotoxicity of ketamine here and the neurotoxicity of amphetamine here. SSRIs can sometimes lead to long-lasting emotional blunting and PSSD.
- What is the effect of the medication on how the person uses her brain? For example, in depression, many people ruminate constantly instead of having more productive lines of thought. Over time, if depression is lessened, using one’s brain in more complex ways other than rumination will have positive second-order effects on brain structure and function.
- What is the effect of the medication vs. no medication on the individual’s lifestyle (e.g., sleep, exercise, nutrition, substance abuse)? For example, some antidepressants mess with sleep and or increase appetite, which will both have adverse long-term effects on brain health.
- Anything that lessens depression & anxiety has a pro-social effect and being social is incredibly good for the brain given that our superb brain probably evolved because we were so social for millions of years (the social brain hypothesis). Asociality & loneliness are highly associated with dementia.
- Similarly, anything that lessens depression & anxiety reduces substance abuse, which is often highly neurotoxic (weed is discussed here; opioids here; MDMA & cocaine & meth here).
- What is the effect of the medication on the individual’s life situation (e.g., relationships, work, traveling, etc.)? Depressed individuals may self-isolate, which is very bad for brain health given that environmental enrichment (the opposite of isolation) is quite neuroplastic and neuroprotective.
All of these will have independent effects on brain health.
Regardless, even if neuropharmaceuticals were neurotoxic, this is not necessarily a reason against them. Firstly, your life is now. Time in this universe is limited and it is a waste to spend it depressed. Secondly, what you create/do now, will have long-term effects on your life. Stark example. If you hop on amphetamines now, even if they are neurotoxic, and lay the foundation for a future career, a small tradeoff with brain health may still have been worth it.
A word of warning
As I had to learn the hard way, drugs that alter neurobiochemistry are nothing to be played around with. While I can certainly have a valuable learning experience, under the influence of the “wrong” neuropharmaceutical I can also do a lot of harm to my own life and the life of those around me. Just as other kinds of tools, antidepressants are still tools.
Thoughts on modern psychiatry
I share my thoughts on and criticism of modern psychiatry here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Part III: Lifestyle & general interventions
Even though this article is called “What Kind Of Antidepressant Should I Choose?” I feel that a couple of non-antidepressant tactics & strategies are worth mentioning.

Exercise
I would have to be some special kind of stupid to take an antidepressant without first trying regular exercise. There is more than enough data to conclude that consistent exercise has an effect size almost comparable to the benefit of medication and psychotherapy, at least in “light” cases of depression.
An exercise regimen can work wonders for vitality, the opposite of depression.
I would particularly focus on endurance training (at least 2-3 hours per week) and less on strength training because endurance training boosts neurogenesis and monoamine regulation more than other forms of exercise.
My nervous system is the basis of everything I think, do, and feel, and few things improve it as much as regular exercise.
For the scientifically inclined:
- In the short term, exercise stimulates monoamine transmission for a couple of hours. Affected monoamines particularly include serotonin and noradrenaline. Furthermore, intense exercise leads to a prolonged upregulation of the “feel-good” mu-opioid system as a counterregulatory mechanism to the activation of the “feel-nasty” kappa-opioid system, which is activated during intense exercise. These short-term changes in neurotransmitters are the major reason why “you are only one workout away from a good mood”.
- Exercise stimulates the release of nerve growth factors such as BDNF & VEGF. In fact, it seems to be one of the most neurogenetic interventions available to mankind – endurance exercise more so than resistance training. HIIT exercise is even better.
- Regular vigorous exercise also promotes cell proliferation in the hippocampus, which enhances mood, memory, and cognition. In part because of this, exercise is probably among the most powerful tools to stave off cognitive decline.
- Exercise stimulates the locus coeruleus, the brain’s major source of noradrenaline, and causes this collection of cells to increase in size and baseline activity (which can be seen as a grey matter increase in an MRI). Therefore, over time, exercise really does lead to a more alert brain, and the reason is a long-term structural change (or better, a combination of multiple structural changes).
- Exercise increases brain oxygenation and improves sleep, both of which are crucial to brain health.
The beneficial effects of exercise on the human brain, and my personal exercise regimen, are discussed here.
Sleep
Similarly, I would have to have been living under a rock if I had not heard about the beneficial effects of sleep, which has a bidirectional relationship with mental illness. There are a variety of strategies, tools, and molecules that are helpful for improving sleep.
I discuss my approach to sleep optimization here. Hypnotics are discussed here.
Blue light exposure
I use blue-light emitting glasses for 10-15min after waking up (discussed here).
In the short term, exposing oneself to bright light (particularly in the morning hours) stimulates cortisol release (high morning cortisol is a good thing). Furthermore, through direct retino-raphe projections, bright light also elevates serotonin signaling.
The increase in cortisol combined with an increase in serotonin transmission helps with energy and mood for the coming day. Bright light is thought to also affect the dopaminergic system.
In the long run, regular exposure to bright light (particularly in the morning) synchronizes circadian rhythm, potentiates the cortisol awakening response (CAR), improves levels of various neurotransmitters, and improves body temperature patterns. These effects are sustained even if I stop exposing myself to bright light for a few days because of a better entrained circadian rhythm.
Diet
Two friends of mine had success with the ketogenic diet in terms of improving their mental health, though I personally was harmed by it. At the very least, if I were depressed, I would make sure to avoid eating too many processed foods and sugar. I would also watch my calories closely as both overeating and undereating can make the depression worse. Some people find the carnivore diet helpful.
I discuss my approach to diet in more detail here.
Stress reduction
Scientific evidence and anecdotal experience suggest that depression is worsened by stress. I would implement different strategies for stress reduction, particularly mindfulness meditation and gratitude journaling. Both of these practices have quite some solid scientific evidence backing their usefulness.
Cold & heat exposure
Some people find value in cold exposure, which stimulates catecholamine levels (dopamine & noradrenaline) and possibly also modulates the immune system. The increase in catecholamine levels has direct antidepressant effects, though short-lived.
Some people also find value in heat exposure (sauna), which stimulates the serotonergic & mu opioidergic system, upregulates heat shock proteins (whose therapeutic benefit is still disputed), and potentiates growth hormone release. Furthermore, regular heat exposure mimics some of the effects of low-level exercise.
Routine
If I were depressed, I would very likely benefit from creating (and sticking to) a daily routine.
Ruling out common causes of fatigue
Chronic fatigue and depression have a partially shared underlying neurobiology, and both can be mistaken for each other. I discuss this in more detail here: „I Am Tired All The Time“ – 12 Overlooked Reasons For Fatigue
Avoiding recreational drugs
Even though tens of millions of people around the world use recreational drugs to temporarily “cure” their unhappiness, eventually they make things worse, in part because after every “up” there is a “down” (due to the principle of counterregulation), and in part, because they are not very helpful to improve things that need improvement.
I discuss the downside of various recreational drugs here: weed (here), amphetamines (here), cocaine (here), MDMA (here), methamphetamine (here). Psychedelics are an exception (discussed shortly).
However, coming off is often hard, particularly in light of depression. I discuss this in more detail here: Kicking Addictions – Potentially Helpful Agents
Purpose & human connection
“And just like a beaver must build a dam to truly express his beaverness, humans must form social bonds to fully express our humanity.” Or as Johann Hari puts it, just like bees evolved to live in a hive, we humans evolved to live in a tribe. If we disband our tribes, we pay a price.
Therefore, evolutionarily speaking, belonging to a tight-knit group and having deep connections with others was (and still is) of existential importance to humans. When a human being lacks it, the brain evolved to respond with feelings of distress (loneliness) in the same way it evolved to respond with feelings of hunger and thirst whenever there is a shortage of food or water.
In a similar way that hypothalamic cells measure energy intake and determine appetite vs. satiety (POMC neurons), new research suggests that there is something similar for regulating “social satiety”, including “rebound socialization” after prolonged social isolation in rats.
Depression (particularly male depression) is often due to a lack of purpose or a “mission”. Similarly, for both genders, a lack of human connection seems to be quite prevalent (and causal).
If both purpose (a “mission”) and human connection could be given “in a pill”, very few people would need antidepressants ever again. Unfortunately, they cannot be bought or prescribed but they must be earned. Even more unfortunate, depressed people rarely have the necessary energy, mood, and motivation to put in the work to earn them. Focusing on vitality first is a good starting point.

I discuss purpose and human connection in more detail here.
Blood tests & hormones
If I were depressed, I would also do a blood test to check for inflammatory markers (e.g., CRP, fibrinogen), markers of metabolic status (e.g., OGTT), and most importantly, I would check for hormone deficiencies.
I discuss my approach to blood testing in more detail here.
Hormones deserve a special mention. If one or more of my major hormones were deficient, as judged by lab results and clinical signs & symptoms, I would research why it may be deficient, and try lifestyle interventions first. If lifestyle interventions do not cut it, I would consider hormone replacement therapy.
Thyroid hormone deficiency is associated with increased rates of depression and thyroid hormones are sometimes used by psychiatrists as an augmentation strategy even if thyroid hormones are not deficient. T3 seems to be more effective than T4.
Similarly, deficiency in sex hormones (primarily testosterone & estradiol) is associated with increased rates of anxiety & depression in both males and females, and sex hormone optimization is an effective (but potentially unsafe) way to treat depression & anxiety.
A friend of mine with recurring bouts of depression has tried out pretty much every antidepressant under the sun. The only thing that sustainably worked for him was a supraphysiological dose of testosterone, which though is potentially unsafe to take in the long term.
Similarly, both leptin deficiency, as well as growth hormone deficiency (and the resulting deficiency in IGF-1), are associated with a lack of vitality and depression. However, growth hormone and leptin are rarely used therapeutically to treat depression. Furthermore, both of these hormones are expensive and hard to come by, particularly recombinant leptin.
I discuss these hormones, and my personal experience with them, in much more detail here.

The downside of hormone optimization for depression is that hormones do not just treat the nervous system (the organ of origin for mental health issues) but every other organ as well. While this is desired in case of hormone deficiency, which has systemic effects, exposing the whole body to supraphysiological levels of hormones is potentially unsafe in the long run.
Making life changes
More often than not, people who are depressed have something wrong with their lives, and quite often depression is a consequence of that. There are exceptions, but most people aren’t them.
Even if we managed to uncover the precise neurological underpinnings of depression, and managed to effectively reverse this state, it is possible (and even probable) that many people would still not be “happy”.
While people might be able to feel more joy, in the opinion of Daniel Kahneman, what people really want when they talk about happiness is being content with the circumstances of their life and having a life worth living (life satisfaction), which requires much more than just biochemical well-being.

Therefore, in many cases, sustainable improvement is contingent on making real-life changes. Sometimes there is an obvious thing that needs to get done, such as cutting ties with assholes, finding new friends, opening up to others, leaving a bad relationship, changing one’s job, or dialing back on work. Other times, it is much harder because dead people can not undie, or one’s family of origin cannot be changed.
Unfortunately, most humans cling to what is familiar and many resist any deviation from what they know. Making changes is usually perceived as uncomfortable because humans do not like uncertainty – particularly in a state of depression. However, to deal with depression sustainably, there is usually no way around making non-trivial changes, even if they are uncomfortable to make.
Psychotherapy
While biological augmentation may be quite helpful (and can often catalyze a gradual shift in perspective and agency), psychotherapy can be immensely helpful for addressing non-biological components of depression.
Therapy is like getting a good second opinion on one’s life from a professional. Therapy may help people with “reframing” things (editing the narrative/story people tell themselves). Moreover, it may help with realizing what life changes need to be made, and ideally, then help people with making these changes.
There’s a saying in therapy: “Insight is the booby prize of therapy.”, which means that the client can have all the insight in the world but if he/she does not make changes in the real world, the insight is not worth much (though it may help a little with “reframing” things).
A special kind of therapy, is taking psychedelics. Psychedelics have powerful perceptual effects (”a year´s worth of psychotherapy in one afternoon). Among other things, they help with getting some “deathbed clarity” before deathbed happens so people can actually do something about it. Furthermore, it may help people with feeling more connected to others and/or with finding purpose in life.
For example, when a friend was working with psychedelics, he often had great insights. However, for him, even seemingly life-changing conceptual insights usually did not lead to any significant long-term change by themselves. Unless he really tried to implement his insights, he was usually back to autopilot a couple of weeks after his trip.

Why would I need therapy if depression is caused by a “brain disease”?
Well, etiology and pathophysiology are not the same. I need lifestyle or antidepressants to change neurotransmitters, neurogenesis, and gene expression (pathophysiology), but I need therapy because some things in my life, or the way I view things, are not the way they should be (etiology), which in many (but not all) cases is the root cause of the pathophysiological changes associated with depression.
Several studies have shown that for people with a history of childhood trauma particularly, the benefits of therapy are greater than the benefits of medication.
There are some meta-reviews about what kind of psychotherapy is best, though, it seems that the results mostly depend on the previously held “conclusion” of the authors that conducted the review. It is thought that the patient-therapist relationship is by far the most important ingredient for successful psychotherapy and much more important than the specific kind of psychotherapy.
Unfortunately, most insurance companies do not pay for therapy, in part because it would be much more expensive than medication, and in part, because it may be abused by people to get therapy for free.

The mind has powerful top-down effects
I like to divide factors that influence my mind into “bottom-up” and “top-down”.
“Bottom-up” factors are any biochemical changes that influence my mind, including neuropharmaceuticals, sleep, exercise, and hormones. (Most of my blog is about bottom-up effects.)
“Top-down” factors are primary mental changes which then influence neurobiology.
As explained in my article on depression, two of the leading theories on depression are the “stress hypothesis” hypothesis and the “rank order hypothesis”.
The stress hypothesis of depression
Some researchers believe that biological depression may have evolved as a protective mechanism to prevent people from running themselves into the ground. According to this theory, prolonged stress triggers the neurobiological cascade biological depression (a downward deviation from baseline) to “help” individuals let go of unattainable goals and/or withdraw from desperate situations.
If an individual’s energy and mood deteriorates the animal is more likely to let go and withdraw. Conversely, if an individual’s energy and mood did not deteriorate, she might continue to overexert herself and die. Indeed, prolonged stress and a perceived effort vs. reward imbalance seems to be one of the greatest risk factors for developing depression.
The rank-theory of depression
Some researchers speculate that depression may have proved useful in dominance conflicts that are unlikely to be won. According to the “rank theory of depression”, sustained melancholy, withdrawal behavior, and a fixation on personal shortcomings and insufficiencies may ensure that the weak “keep their heads down” and don’t overreach themselves, which may prove evolutionarily fatal.
The rise of depression and anxiety in young people coincides with the advent of social media, and there is probably a causal connection at play. Social media constantly floods people with “evidence” that many others have it better.
According to this theory, depression may represent a fitness-enhancing adaptation to group living. Indeed, if individuals are “losing” in life, they are more likely to develop depression to ensure that they do not get “terminally mauled” or ostracized by more popular group members.
In support of this may also be the fact that adolescents are often depressed (because most adolescents are not on top of the hierarchy – aka the cool kids).
Where I am going with this
While not mutually exclusive, both of these theories are fundamentally related to top-down processes (i.e., thoughts).
Let us assume you are in a foreign country, travelling and you have no way of communicating with anyone. I then let you know that your whole family died in a car crash. The neurobiological cascade happening from this information, far more extensive than a simple rise in the HPA axis and cortisol secretion, can lead to true neurobiological depression, including a reduction in neuroplasticity and large scale changes in gene expression.
Similarly, a decade ago, I used to be semi-depressed for about half a year or so because I was reducing myself, my thoughts, and my feelings to molecular biology. Then, simply learning about the concept of emergence was quite powerful in terms of boosting my liveliness for many months – I remember it vividly to this day. In other words, I boosted my liveliness from “within” the mind. I would assume that among other things, my neuroplasticity and monoamine signaling were somehow altered.
Analogously, let us say you think you are the biggest loser around. You then take a psychedelic drug (or go to therapy or whatever) and now you gradually start to believe deep down that you are actually amazing. Your neurobiology will reflect that in the same way that there are profound hormonal changes (e.g., cortisol, testosterone) if certain species of monkey perceive themselves to be on the top vs. bottom of the hierarchy. In fact, quite a bit chunk of our brain is frequently occupied with hierarchy calculation & negotiation and for the hypersocial animals we are, it does make evolutionary sense that a lot of your operating system is reacting fundamentally to your perceived standing in contrast to others.
The placebo effect is another prime example of a top-down effect. The placebo group in antidepressant studies usually measurably improves in a variety of domains. Similarly, being hopeful or simply believing in something can have measurable physio-biochemical ramifications.
Children who are mistreated or neglected sometimes fail to thrive (to grow properly). This form of “psychosocial dwarfism” can occur even when adequate caloric intake is provided.
In orangutan tribes (orangutans are somewhat closely related to humans), there is only one alpha male and something about the sheer presence of an alpha male has other male orangutans growth-suppressed (it is thought that his screams play a role). After the alpha male dies, the growth-suppressed young orangutans suddenly go through puberty. This means that puberty was induced purely from “within the mind”.
In all of these examples, profound changes are happening throughout the brain and consequently body even though in every instance this is only information without any real-world correlate.
It should be easy to see where I am going. If people are constantly comparing themselves on social media to people who have it better and/or ruminating on their shortcomings and/or do not feel connected to others, real biological changes set in simply from a thought-based origin – it does not matter whether these thoughts are rooted in reality or not. This is why lying to yourself (if you are able to pull it off) is so powerful.
Consequently, techniques that change your day-to-day thoughts are super effective in changing your liveliness – and not just on a “conceptual” level.
Among these techniques:
- Gratitude practice: We humans have a negativity bias and we dwell more on the things that are not going well compared to the positive things which we often take for granted. A gratitude practice can counteract this somewhat. Over time, as you get “better” at gratitude, spontaneous thoughts of gratitude come on more readily in the same way you start to see red-haired people everywhere once you have trained your pattern-recognition machinery jammed between your ears to spot them.
- Meditation: Many negative thoughts come on spontaneously, often while we are doing something else. The stupid practice of paying attention to your breath then helps you notice these negative thoughts once they come up (vs. being lost on autopilot and getting carried away by them). Furthermore, in the same way muscle strength is automatically transferred to daily life if you lift weights, your baseline concentration during daily life improves if you practice meditation and you mind-wander less automatically. In this vein is meditation can stop the rumination mill, which then has real neurobiological ramifications.
- Therapy: Psychotherapy or psychedelics can be really effective as they help you edit the story you tell yourself (e.g., you see that you are not as pathetic as you thought you are, etc.).
The main point of this entry is basically that vitality can be quite deeply affected by not just changes that are bottom-up (e.g., altering hormones or neurotransmitters trough lifestyle of exogenous molecules – which is what my blog is mostly about) but also by more “psychological” changes (i.e., information), which eventually affect deep material processes within the brain including individual neurons.
While this may seem “duh” to most people, for me, a biological materialist at heart, this was quite eye-opening to find out about – even though the biological mechanisms are far from being elucidated.
(It obviously also goes the other way: If my neurobiochemistry changes (e.g., from hormonal changes, lifestyle changes, or medication), then my thoughts and outlooks also change – something that I extensively discuss elsewhere.)
Other articles on depression
Sources & further reading
- Website: Wikipedia – Biology of Depression
- Anecdotes: Reddit – r/depressionregimens
- Website: Wikipedia – (Useful) List of investigational antidepressants
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.