
Metabolic drugs can have a powerful impact on metabolic health, which is key to longevity. Metabolic drugs affect key molecular pathways including insulin/IGF-1, mTOR, and AMPK pathways, which have all been extensively studied in the context of longevity and are key candidates for extending health span and lifespan. Nutrient-sensing pathways are presumably more important for delaying aging than reversing it.
I will now discuss a couple of these drugs in more detail and describe my experience with them as a metabolically healthy person.

Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Acarbose – a “slow-carb” diet in a pill
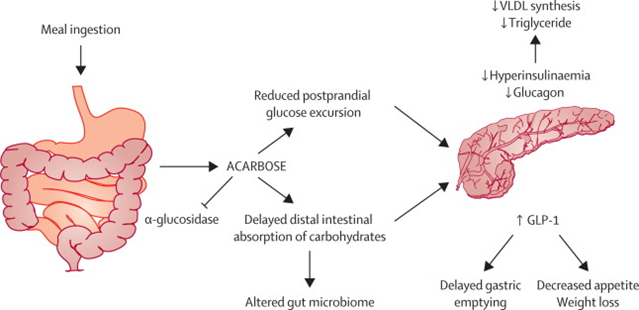
Acarbose is a glycosidase inhibitor. Alpha-glycosidase is an enzyme responsible for breaking down starches into simpler sugars. This delays the digestion of carbohydrates, essentially transforming “bad carbs” into “good carbs”.
In simple terms, when acarbose is taken with a meal, fast-spiking carbohydrates (“bad carbs”) are converted into slow-release carbohydrates (“good carbs”). This reduces carbohydrate absorption, blood glucose peaks, and area-under-curve levels of insulin, and elevates levels of GLP-1.
However, the price to pay is flatulence and diarrhea (especially initially). I stopped taking acarbose because even low doses (25mg) consistently elevated my liver enzymes, which is a rare idiosyncratic reaction.
There seems to be something harmful about large glucose spikes and they seem to be associated with all kinds of bad long-term consequences, including a reduction in lifespan. Some researchers speculate that large glucose spikes trigger something “bad” within the hypothalamus.
Interestingly, acarbose is one of the few molecules that increases lifespan in male mice, as evidenced by the results of the Intervention Testing Program (ITP), a program designed to identify molecules that prolong lifespan and health span in mice.
In the Intervention Testing Program, acarbose prolongs median lifespan of male mice by a whopping 22% across all 3 test sites – and it prolongs maximum lifespan by 11%. It is much less effective in females. Acarbose is one of a handful of molecules that ever passed the ITP. Interestingly, many of them are metabolic drugs.
It is thought that the lifespan benefits of canagliflozin (an SGLT-2 inhibitor) or acarbose (a glucosidase inhibitor) likely come down to, at least in part, a blunting of peak glucose levels. The only other molecules that led to significant lifespan extensions were rapamycin, canagliflozin (SGTL-2 inhibitors are discussed shortly), alpha-estradiol, and astaxanthin (the only OTC molecule). Unfortunately, senolytics have not yet been properly tested.
Acarbose is extensively used in Asia but for some unexplained reason, it is rarely used in the West.
Acarbose is effective for reactive hypoglycemia (getting ravenously hungry due to blood glucose swings shortly after eating).
Metformin – short-term fasting in a pill
A couple of years ago, I took metformin on the premise that there is little risk to it.
I started with only 500mg of extended-release metformin per day and increased by 500mg every week until I reached my target dose of 3x500mg per day, which I had been taking for about a year or so.
In my first month, there was some tiredness and nausea. Thereafter, there were no adverse effects. However, throughout my time on it, I occasionally had some bloating and gut issues, which I erroneously blamed on the microbiome.

Somehow (perhaps by inhibiting proteins in the electron transport chain), metformin skews the ratio of AMP/ATP and thus tricks the cell into believing that there is an energy shortage, thereby activating AMP-kinase, which switches off many ATP-consuming pathways such as gluconeogenesis, protein synthesis, and fatty acid synthesis, and turns on ATP-generating pathways such as beta-oxidation (the breakdown of fatty acids for energy) and glycolysis (the breakdown of glucose for energy). The activation of AMPK also increases insulin sensitivity..
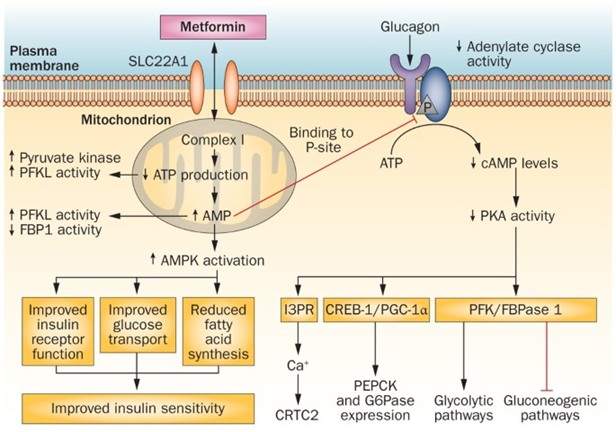
Furthermore, AMPK is thought to stimulate mitochondrial biogenesis and autophagy. Somehow, due to all of this (or due to some other effect), metformin is known to also reduce levels of inflammation.
All of these effects are quite similar to the effects of caloric restriction, weight loss, or intermittent fasting – but “in a pill”.
However, as I did more research, I realized that while metformin is useful for combatting insulin resistance, metformin is not the “free lunch” that it is made out to be in individuals who are already metabolically healthy and the downsides may outweigh the upsides:
- Many researchers consider metformin to be essentially a mitochondrial toxin, evidenced by the fact that it increases lactic acid levels at rest.
- Metformin blunts some of the beneficial responses to exercise, in particular the post-exercise inflammation (which is beneficial) and the exercise-induced upregulation in antioxidant systems.
- Metformin leads to an increased expression of hydroxysteroid-dehydrogenase II, the enzyme responsible for converting cortisone to cortisol. This causes tissue levels of cortisol to increase, which is bad for a number of things.
- Metformin decreases the activity of POM-C neurons. POM-C neurons are central integrators of energy availability and energy expenditure.
- Metformin puts people at risk of vitamin B12 deficiency.
- For some people, metformin causes bloating and gut issues.
Even though in the Intervention Testing Program (ITP) metformin alone did not increase lifespan, metformin plus rapamycin (discussed shortly) has increased the average lifespan of mice by 23% – the longest-living animals so far in the ITP.
I now use metformin as part of my Long-COVID prevention protocol. In overweight individuals, starting metformin shortly after contracting COVID reduces long COVID incidence by roughly 40%.
Rapamycin – prolonged fasting in a pill
Rapamycin is a highly potent and selective inhibitor of mTOR, which is one of the major “growth”-pathways in eucaryotic organisms. The most powerful (natural) way to turn off mTOR is to fast. Rapamycin is the best fasting-mimicking drug currently available. Furthermore, it is the only drug that extends lifespan in all animals it has been tested so far.

Rapamycin has profound effects on metabolism. It stimulates lipolysis & beta-oxidation and increases ketogenesis. It also reduces the accumulation of senescent cells, lowers inflammation, and enhances mitophagy.
Over the past 5 years, I have taken 3-6mg of rapamycin once weekly. At this dosage, for me, there are no deleterious effects on insulin sensitivity, fasting blood glucose, or lipid levels (after the initial couple of months had passed). I discuss the science and my experience with rapamycin in more detail here. I always stop taking it in the winter months because it does make me more susceptible to infections.
SGLT-2 inhibitors – a low-carb diet in a pill
As mentioned in the section on acarbose, interventions that control daily peak glucose levels deserve attention as possible preventive medicines to protect from a wide range of late-life neoplastic and degenerative diseases. SGLT-2 inhibitors are among the most powerful drugs currently available to improve metabolic health.
For some unknown reason, these molecules are among the most organoprotective molecules known to mankind. Even though they have very little effect on blood sugar levels (incl. HBA1C levels) they paradoxically reverse aberrant glucose metabolism more than other classes of drugs that have a strong effect on blood sugar (such as metformin, sulfonylureas, insulin, etc.).
It is hypothesized that the steady excretion of glucose leads to a more fat/keto-adapted metabolism. It is further hypothesized that this switch from “metabolizing sugar for cellular energy” to beta-oxidizing fatty acids and ketones for cellular energy is at the very center of organ protection and tumor prevention.

SGLT, standing for Sodium-Glucose-Transporter, is a protein that absorbs glucose from the outside of the body (such as the intestine and kidney tubules – both of which are technically outside of the body) and shuttles it into the body. SGLT-1 is mostly expressed in the intestine, while SGTL-2 is the predominant glucose-reabsorbing protein in the kidneys, where it is responsible for about 90% of renal glucose reabsorption (about 50-100g/d – depending on one’s kidney function and blood glucose levels).
If SGLT-2 is fully blocked, on average about 60-90g of glucose is lost via the urine per day. This urinary loss of glucose not only results in the loss of about 300-400kcal per day, but it is also responsible for a host of beneficial metabolic effects.
Most importantly, through some yet unexplained mechanism, cellular metabolism shifts towards a more fat-adapted state, and blood ketone levels become slightly elevated – so essentially some of the benefits of a low-carb diet but in a pill.
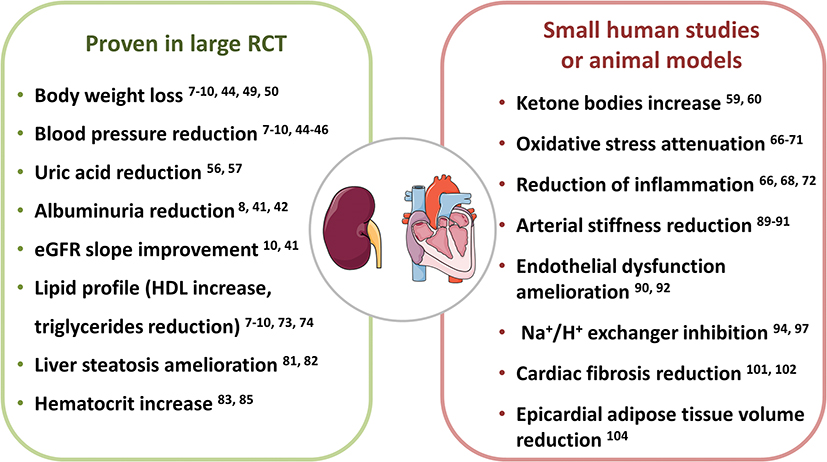
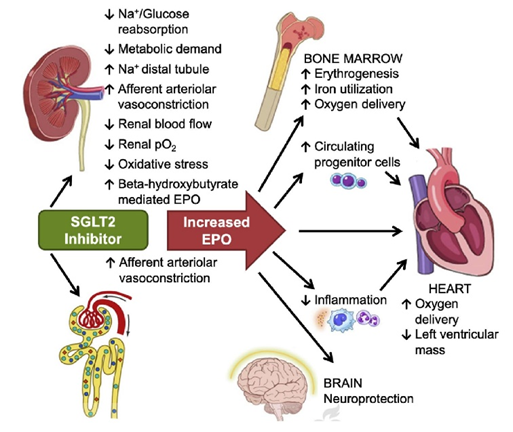
Blocking SGLT-2 leads to an increase in insulin sensitivity (and everything that entails). Because of this, SGLT-2 inhibitors are beneficial for a wide range of age-related disorders, including cardiovascular disease, cancer, and presumably also neurodegeneration. There is good data that SGLT-2 inhibitors also have nephroprotective, cardioprotective, and antineoplastic effects that are independent of insulin regulation.
For me, the selling point was their effects on EPO regulation. Because of a complicated mechanism, SGLT-2 inhibitors increase EPO levels, which raises RBC count. Thus, SGLT-2 inhibitors are a safe and elegant way to increase my hematocrit by a few points.
However, the loss-of-glucose-induced natriuresis also has a diuretic effect comparable to thiazide diuretics and therefore lowers blood pressure (which is, for most people, a good thing).
On SGLT-2 inhibitors, I needed to pee a lot, which I find distracting. Furthermore, they dehydrated me, my eyes got dry and my voice got breathy. Because I did not seem to adapt to these effects to a meaningful degree, I decided to stop taking them despite their numerous known benefits.
It is worth mentioning that SGLT-2 inhibitors are also one of the few drugs that effectively prolonged lifespan in mice in the Intervention Testing Program (ITP) by the National Institute on Aging. More specifically, canagliflozin increased the lifespan of male mice by 14%. Interestingly, the lifespan of female mice was unaffected.
In sum, SGLT-2-inhibitors have pleiotropic effects on longevity, including a blood-pressure-lowering effect, EPO-induction, ketone body formation, a reduction in uric acid levels, lipolysis, anti-inflammatory and anti-oxidative effects, and a potent increase in insulin sensitivity. I believe that SGLT-2 inhibitors will eventually replace the use of metformin for most purposes.
Semaglutide
Semaglutide is a GLP-1 agonist. Because the GLP-1 receptor is expressed in many different tissues and brain sites, GLP-1 agonists have a plethora of different effects. Including:
- Appetite reduction (via two or three independent mechanisms)
- Loss of body weight (partially independent of their appetite-regulating effects)
- Improvement in metabolic health (partially independent of the above effects)
Furthermore, they slow the progression of diabetic kidney disease, reduce cardiovascular events, and help with non-alcoholic steatohepatitis (NASH). I find it most fascinating that, according to currently available data, they may delay the onset of dementia. Furthermore, anecdotally, they seem to have broad-spectrum anti-craving effects (not just limited to food cravings).
For most people, semaglutide increases metabolic health because it leads to a loss of body fat, which increases insulin sensitivity. Some people worry that they decrease muscle mass. Personally, I have built about 3 kg of muscle on semaglutide, though I also started doing CrossFit at about the same time.
Semaglutide is one of my favorite drugs. However I stopped taking it – I discuss the science and my personal experience with it in detail here.
Allopurinol
I take allopurinol because I have a couple of deleterious SNPs in my URAT1 and my uric acid levels naturally hover around 7mg/dl, which is right about the concentration where uric acid starts to precipitate in a number of tissues in the form of needle-like crystals.
These urate crystals are thought to cause low-level inflammation, potentially worsening tissue health in several organs (much more than just gouty joints). The ensuing renal inflammation is also thought to increase the activity of the RAAS system and therefore to elevate blood pressure.
On the other hand, uric acid is also an antioxidant, and about half of the blood’s antioxidant capacity is due to uric acid. Therefore, I try to keep my uric acid in a low normal range of 4-5mmol/l. To achieve this, I use 100-150mg of allopurinol per day.
Hormones
Technically, exogenous hormones are metabolic drugs as well. The following hormones affect metabolism, nutrient partitioning, and body composition, all of which are central to metabolic regulation.
Furthermore, regardless of their direct effects on cells and tissues, hormones have powerful effects on energy levels, mood, well-being, cognition, vigor, and vitality, which make living a “healthy lifestyle” much easier.
- Thyroid hormones regulate “metabolic speed”. Thyroid hormones increase the general rate at which metabolic processes are happening and therefore their effects can either be anabolic or catabolic, depending on caloric intake and the presence of anabolic hormones. Generally speaking, hypothyroid individuals have a hard time losing weight, while hyperthyroid individuals lose weight easily.
- Cortisol prepares the body for action. It stimulates gluconeogenesis & lipolysis and turns off anabolic pathways. In the short term, cortisol is very catabolic to everything while in the long term, cortisol remains catabolic to everything but, for some reason, is anabolic to fat tissue in the face (“moon face & buffalo neck”) & trunk.
- Sex hormones regulate nutrient partitioning. Among other things, testosterone is anabolic to muscle and catabolic to subcutaneous fat, while estradiol stimulates the deposition of subcutaneous fat (presumably to prepare the organism for pregnancy). The sex-hormone-mediated increase in lean body mass increases insulin sensitivity.
- Low levels of leptin prepare the organism for starvation. In its absence, the release of other hormones (except for cortisol) is vastly reduced. Furthermore, what is not known to many, leptin directly regulates the metabolism of the liver (metreleptin treatment is known to help with NASH). Furthermore, there are leptin receptors on muscle cells and fat cells, which comprise about 80% or so of body mass. I discuss my experience with leptin here.
- Insulin is the central master regulator of metabolism. Insulin deserves its own article and I discuss insulin in detail here.
I have experimented with all of them (except for pure IGF-1), though I only currently take a low dose of a low dose of metreleptin at the moment.

I discuss my experience with some of these hormones in more detail here.
My current approach to metabolic drugs
At the moment, I only take a low dose of metreleptin and a low dose of allopurinol.
I stopped the semaglutide because it made it impossible to gain weight. I stopped the rapamycin because I am waiting for more human data.
If I had to choose drugs for diabetes
In my opinion, first-line drugs should be GLP-1 agonists, as they address the core issue of diabetes. Firstly, they lead to weight loss, and the loss of visceral adipose tissue increases insulin sensitivity. Secondly, they change insulin levels by acting on the hypothalamus (more specifically, POMC/CART neurons), which has drastic effects on blood sugar levels through direct vagal control of the pancreas, liver, and other tissues. So, GLP-1 agonists mostly work through the brain by affecting CNS control of metabolism (including insulin release) and appetite levels.
SGLT-2 inhibitors are amazing drugs, also. However, unlike GLP-1 agonists, they do not address the core of insulin resistance (visceral fat; faulty brain circuits) and are therefore inferior to GLP-1 agonists.
What about combining metabolic drugs?
The drugs mentioned above can, in theory as well as in practice, be combined in a mix-and-match fashion. Furthermore, most of these drugs can be combined with most diets (a possible exception being combining SGLT-2 inhibitors with very low carbohydrate diets because that vastly increases the risk of ketoacidosis – however, one of my best friends effectively combines the two but he monitors his urinary ketone levels daily).
However, given that certain diets (e.g., ketogenic diet, fasting-mimicking diet, intermittent fasting) and certain drugs have partially overlapping mechanisms, and eventually converge on the same intracellular signaling hubs (e.g., AMPK, mTOR), their combination is, in most cases, less than additive, and definitely not synergistic.
Are metabolic drugs necessary?
Many but not all benefits of these drugs can be obtained by smart dietary and lifestyle choices alone. However, some of the same signaling cascades that are activated by lifestyle choices can also be manipulated pharmacologically.
In principle, my cells could not care less whether downstream signaling pathways are activated by lifestyle choices or pharmaceutical intervention. I discuss my thoughts on the “ethics” of intervention in more detail here.
Thus, antidiabetics can also be used by “normal” people as metabolic enhancers – and there is quite some data that these drugs improve general health on many fronts (e.g., rates of atherosclerosis, cancer, or dementia decrease).
Sources & further information
- Podcast: Peter Attia & Richard Miller: The gold standard for testing longevity drugs: the Interventions Testing Program
- Podcast: Peter Attia & Ronesh Sinha – Insights into the manifestation of metabolic disease
- Scientific article: Novel Insights into the Roles and Mechanisms of GLP-1 Receptor Agonists against Aging-Related Diseases
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.