
I recently coached a client. From the outside, he appeared to be very fit. He had chiseled six-pack abs, exercised every day, and was very health-conscious. However, for the past couple of years, he had issues with energy levels and recovery. He also felt quite weak most of the time and his blood pressure (around 110/60) and resting heart rate (around 50) were “elite”. His hands and feet get cold easily. His libido was okay-ish. His emotionality was low. His complexion was pale.
To help with energy levels, another doctor put him on a high dose of thyroid hormones, which he had been taking for years. This somewhat helped, particularly initially, though after some time he started to feel fatigued again. His TSH got completely suppressed already on a much lower dose, a dose that should not have suppressed him.
His total testosterone was decent, though artificially elevated because of the high SHBG, which was sitting slightly above the reference range. His LH, FSH, and free testosterone were borderline low, and his estradiol was below the reference range. Many “functional” doctors would blame his subpar sex hormones for his symptoms, though that is only part of the story.
He also had reactive hypoglycemia, meaning that he feels hypoglycemic 1-2 hours after eating.
Another anecdote. I recently dated a who has had amenorrhoe for 2 years. She also had cold hands and feet and a blood pressure of 105mmHg. Her SHBG was high. Endocrinologists did not know what was wrong with her though releasing-hormone tests had shown that her amenorrhoe was hypothalamic.
She had been to the best university doctors in my country. They ran all kinds of tests on her, including genetic analyses and a number of stimulation tests. But for all their degrees and specializations could not figure out what was wrong with her. She told me that a couple of years ago she had lost about 15kg of fat… Sometimes you do not need to solve complex equations but all you need to do is putting 1+1 together.
Over my years of consulting with a large number of “healthy” individuals (over 100 at this point), I have seen the same syndrome over and over again. Super-fit-looking individual who is very into health and fitness. Physical energy levels of a 60-year old. Low heart rate and blood pressure. Females often present with irregular periods and menorrhagia and sometimes even amenorrhea. Women often have small visible vellous hair below the ears and outer cheeks. Males usually present with testosterone and E2 on the lower side. Often, both genders present with a high SHBG and a low fT3 while their TSH levels are decoupled. Sometimes the symptoms have been precipitated by a ketogenic diet, intermittent fasting, or dieting. Most of them also have reactive hypoglycemia (feeling “weird” and ravenously hungry soon after eating).

Individuals often assume that their “great” blood pressure and heart rate are so “great” because they are so “healthy”. However, their heart rate and blood pressure are so low because their sympathetic nervous system activity is patholgically low, which is presumably also the primary reason for their fatigue. (Note: Contrary to popular wisdom, a lower heart rate is not necessarily better -it is better if the lowering of the heart rate is driven by your heart getting stronger but not if it is driven by a reduction in sympathetic tone).
This syndrome is usually misdiagnosed as hypothyroidism and/or hypogonadism. However, the issue runs much deeper. Hormone replacement therapy helps somewhat, particularly initially (as certain neurotransmitters increase), making individuals think that they have not yet found the holy combination of hormone replacement dials – they experiment with aromatase inhibitors, HCG, progesterone, pregnenolone, Proviron, T3, different macronutrient compositions, fasting, all kinds of supplements, you name it.
Tantalizingly, beneficial changes are short-lived, and they are soon back to a little above square one (as neurotransmitter levels adaptively decline again). I had this weird syndrome myself at one point. Bryan Johnson also has a severe form of it.
What is going on?
Introducing POMC/CART neurons
Many of the symptoms of being in a pre-starvation state (e.g., bradycardia, hypotension, “feeling like shit”, brain fog, tiredness, weakness, etc.) are partially due to a low sympathetic tone. In the brain stem, there are a couple of nuclei that control sympathetic activity. Among them is the locus coeruleus, the major source of noradrenaline (discussed in more detail here).
Baseline sympathetic nervous system activity (different from reactive SNS activity resulting from temporary stressors) is controlled by a variety of inputs. Many of these inputs are hormonal in nature, which is the primary reason people feel better (temporarily) after adding TRT (my experience here), thyroid hormones, or cortisol to their regimen. People also feel better with everything that elevates noradrenaline levels, such as caffeine (in fact, many are coffee junkies), or noradrenergic drugs. In fact, one client who had been on every combination of hormones under the sun got unparalleled relief from bupropion, a noradrenaline reuptake inhibitor with a small effect on dopamine levels. However, the improvement did not last.
A low sympathetic tone explains many but not all of the symptoms of super-fit-super-sick syndrome. For example, issues with thermoregulation, appetite/hunger, and hormones are other issues. The reason is primarily that the hypoadrenergic state itself is only a symptom of something larger.
Sympathetic activity is controlled by various nuclei in the hypothalamus, among them the arcuate nucleus, containing POMC/CART neurons and AGRP/NPY neurons, the primary regulators of energy homeostasis in vertebrate animals (fish, amphibians, reptiles, birds, mammals).
POMC/CART and AGRP/NPY neurons are ultimately responsible for telling the rest of the brain and body that there is sufficient energy availability to spend in pursuit of things other than food. They do this by a variety of mechanism:
- By co-controlling hormonal output of the anterior pituitary gland (HTA, HPA, HTPA). Hence, many of these “fit” individuals have hormonal issues, involving every major hormone system.
- By influencing thermoregulatory processes. Hence, many of these super fit individuals have a pale complexion because the body centralizes blood flow. Many also only feel comfortable within a narrow temperature range and have issues with sweating (thus heat intolerance) and heating up (thus cold intolerance).
- By affecting appetite and nudging cortical areas to think about food-related stuff, many have constant thoughts about food and develop ritualized and obsessive eating habits.
- By affecting personality traits in a way that makes people more likely to acquire food. In humans, this means people become more self-centered, rigid, and obsessive – presumably traits that are intended to help with hoarding and foraging behaviors.
- By regulating sympathetic activity, the latter of which is the major regulator of energy expenditure. Hence, many of these individuals feel weak, have some form of orthostatic hypotension (get dizzy when standing up), have low blood pressure and a low heart rate.
Let us take Bryan Johnson as an example. He has issues with thyroid hormones (of which he takes a very high vastly supraphysiological dosage) and sex hormones, and presumably other hormone systems of which he does not share data. He is the palest person to ever walk the face of Earth, short of albinos (and this goes far beyond him simply avoiding the sun) – though it has gotten somewhat better since he has been going haywire on laser treatments which then artificially improve his complexion via angiogenesis. He is always hungry and has centered his life and identity around eating and not eating. He seems to have gotten quite obsessive, rigid, and self-centered (partially adaptations to foraging). He has a blood pressure of 102/61mmHg (Yikes.). I discuss my thoughts on Bryan Johnson in more detail here.
While he considers (and promotes) these things to be signs of “perfect” health, this is actually a sign of poor health and even poorer vitality. The POMC/CART neurons in his brain get little to no go-signals because his caloric intake, insulin levels, and most importantly leptin levels are all very low. Consequently, his adrenergic tone borders on non-existence, which is also the primary reason behind his “perfect” sleep scores (a low SNS activity causes low heart rate, elevated HRV, low blood pressure, and has people fall asleep instantly). Most people would feel like absolute crap with a sympathetic nervous system activity that low.
I discuss Bryan Johnson in more detail here: The World´s Most Expensive Eating Disorder
GLP-1 agonists such as semaglutide activate POMC/CART neurons, which is presumably the primary mechanism by which these drugs work (their action in the gut such as delayed stomach emptying is probably negligible for weight loss). Indeed, many of these “ultra-fit” individuals feel vastly better on even low doses of GLP-1 agonists. Heart rate, blood pressure, and hormones improve. Sympathetic output soars. Getting hungry soon after eating even “if they do everything right” becomes an issue of the past.
However, even GLP-1 agonists have a somewhat short-lived (e.g., on the order of months) and partial (e.g., mood does not improve) effect because the issue lies even deeper – though much more powerful and “causal” than hormones and noradrenergic drugs. I´ll discuss the practical aspects later.

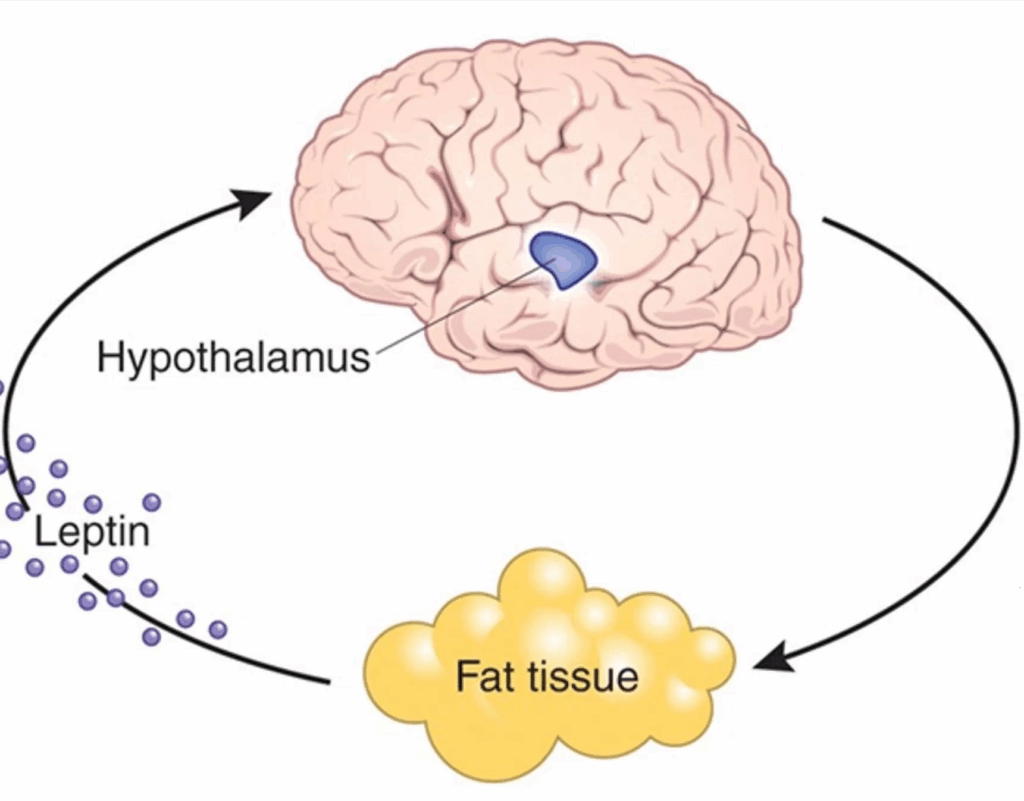
In the image above, it makes it seem that insulin, leptin, and CCK are equivalent regulators of POMC/CART and AGRP/NPY neurons. However, that is incorrect. All three classes of peptides work through very different receptors being coupled to different internal signaling cascades.
- CCK works through a measly G-protein-coupled receptor (GPCR). GLP-1 (and GLP-1 agonists such as semaglutide and tirzepatide) also work through this kind of receptor, as does PYY. All of these are short-term satiety peptides, and their levels are a function of macronutrient intake. CCK is mostly stimulated by fat, PYY is mostly stimulated by protein, and GLP-1 is mostly stimulated by carbohydrate intake. These satiety peptides activate POMC/CART neurons acutely. I discuss GLP-1 agonists in more detail here.
- Insulin works through a receptor tyrosine kinase (RTK), influencing cell activity and cell size. Insulin levels are a function of carbohydrate intake and certain essential amino acids found mostly in animal protein. The important point to understand is that insulin works through a completely different receptor than the short-term satiety peptides discussed above. I discuss insulin in more detail here.
- Leptin works through a cytokine receptor, being directly connected to gene expression changes through a STAT signaling cascade. Leptin levels are mostly a function of body fat levels (subcutaneous adipose tissue expresses more leptin than visceral adipose tissue) and are highly sensitive to short-term weight fluctuations (hence, a “refeed” makes sense when someone approaches single-digit body fat levels). Leptin levels are also influenced by insulin (stimulating), estradiol (stimulating), cortisol (stimulating), and testosterone (inhibiting). I discuss leptin in more detail here.
All of these inputs stimulate activity of POMC/CART neurons though in different ways. However, the most important of these is leptin. Leptin is sort of a “multiplier”. And if you multiply anything by zero, then the product is zero. Indeed, if leptin levels are low, short-term satiety peptides (e.g., GLP-1, CCK, PYY) and insulin do not work as well. If leptin levels are high, it works synergistically with other satiety peptides.
This can be seen in fitness enthusiasts who diet down to low levels of body fat. Even if they “do everything right” nutrition-wise, they find themselves hungry soon after a meal. This also means that leptin has a permissive effect on semaglutide action, meaning that if leptin levels are too low, semaglutide does not work properly. The reason is probably that leptin signaling is coupled to a cytokine receptor (STAT3 signaling) determining the “sensitivity” of POMC/CART neurons. Indeed, the fatter someone is, the better GLP-1 agonists work.
(Of note, in obesity the system is “broken”, possibly due to hypothalamic inflammation, and these neurons are resistant to leptin input, a condition known as “leptin resistance”. GLP-1 agonists are hypothesized to be leptin-sensitizing, which is part of the reason why they work so well in obesity but cease to work properly when individuals reach low body fat levels.)
Because this article is already quite long, for the nerds out there, I explain the subtleties of energy homeostasis in more detail here: Energy Metabolism (Technical Article).
Regulation of POMC/CART neuron activity
POMC/CART neurons are activated in a state of abundance and AgRP/NPY neurons are activated in a state of nutrient deprivation.
POMC/CART neuron activity (which determines weight, appetite, and energy expenditure) is ultimately based on two things: energy intake and leptin levels.
(Of note, in reality things are much more complex and involve a host of neuropeptides and collateral input from adjacent hypothalamic, limbic, and brain stem structures. However, I will keep things simple and in a way that a practical strategy can be derived).
#1: Energy intake
When energy intake remains below caloric needs for a long time, weight-gain-favoring adaptations occur. Such as a lowering of energy levels, mood, sex drive, and satiety. Everyone who has ever been on a diet may have noticed this.
Caloric intake is signaled to the hypothalamus by a plethora of mechanisms. These include satiety-peptides (GLP-1, CCK, PYY, PPY), insulin, vagal nerve endings from the gut, stomach stretch, and hypothalamic receptors for glucose, fatty acids, and amino acids.
GLP-1 agonists can partially hack this (which is why they are so effective for weight loss), meaning that GLP-1 agonists mimic “food abundance”.
#2: Body fat (or more specifically, leptin levels)
When levels of body fat are low (individuals vary with regard to what “too low” means), adaptations to starvation will be set in motion regardless of energy intake. This is single-handedly signaled by the adipokine leptin, which is secreted by adipose tissue in proportion to how “full” an adipose cell is.
This means that if body fat levels (more specifically, leptin levels) are below a certain threshold, the rest of the satiety system ceases to work properly. Unbeknownst to many, the effects of leptin go far beyond appetite regulation.
Of note, leptin levels are highly sensitive to the rate of change. That means, if one is actively losing fat mass, leptin levels will drop much more during the active fat loss phase than what the change in fat mass would predict. Conversely, a “refeed” day can spike leptin levels (as the rate of triglyceride flux in adipose cells is positive). As soon as the fat loss/gain abates though, leptin levels normalize in relation to individual genetics and total amount of body fat mass.
A note on “imprinting”
Some people may find that after a fat loss diet, they do not really recover completely. After losing weight some people develop stubborn energy problem, hormone problems, they feel “like shit”, have cold hands and feet, and their appetite is now ravenous. Colloquially, this so-called state of “starvation mode” sometimes remains for a long time even after the dieting is over (even if #1) energy intake and #2) body fat levels are normalized). This is especially true for yoyo-dieting, where people get progressively worse over time, wrecking their metabolism, hormones, sanity, and health in the process.
Analogous to muscle memory, the energy homeostasis system has some “imprinting” about what had happened in the past. Particularly, times of past starvation seem to be “remembered”. For example, if a mother is in starvation during pregnancy, the child will be much more likely to become obese, partially due to epigenetic imprinting in the leptin system. Other example, 6 years after finishing The Biggest Loser, participants still burned about 500kcal less than what they burned before despite being at the same body weight as before.
It is well known from the literature that starvation has a severe and prolonged effect on sympathetic nervous system activity. It is remarkable that even strictly controlled eating (restrained eating) has an inhibitory effect on noradrenaline secretion. From research on patients with anorexia nervosa it is evident that noradrenaline levels are lower even many years after weight normalization.
After recovering from an eating disorder, some gain weight and seem to recover fully. However, not everyone is so lucky. For some there are persistent metabolic and neuro-endocrine adaptations that never seem to quite reverse even after weight normalization and normalization of food intake. Individuals often (need to) arrive at a much higher fat mass in order to feel similar to where they felt before the eating disorder. The same can probably be said for people who diet down to very low body fat levels for other purposes such as bodybuilding, modeling, etc.

It seems that with persistent dieting there is a stepwise increase in body fat set point happening (probably through POMC/CART neuron reprogramming), meaning that, presumably for evolutionarily obvious reasons, energy/appetite systems in the brain defend against weight loss much more than they defend against weight gain.
It is important to note that this imprinting does not happen to everyone.
It seems, that the brain “remembers” periods of starvation (whether self-induced or otherwise) and that, for many people, these adaptations are quite stubborn and hardly go away. How does this “imprinting” happen? There are two possibilities I can think of. Firstly, on the network level (long term depression or long term potentiation of existing networks). Secondly, on the cellular level (epigenetic alterations in the expression of certain transcription factors in key neuronal population such as POMC/CART neurons).
Currently, there is no strategy or drug available that can permanently lower body weight set point to normal levels – as is evident by the fact that most people who lose weight through a diet (or medication) eventually gain all of it back once stay stop said diet or medication.
In sum, it seems that maintaining body fat much below fat set point for a long time seems to carry long-term risks. Some gain weight and recover fully and quickly. However, I have met quite a few people who did not – some did not even recover after becoming fat. (Of note, GLP-1 agonists only lower body weight/fat setpoint while the treatment is ongoing but as soon as people come off, most of the weight is regained).
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
What is the “cure”?
In the same way people can “live” themselves into obesity, which rarely repairs itself after the appetite/weight system is broken, so might this syndrome of starvation rarely repair itself.
In short, while closest thing to a cure in obesity are GLP-1 agonist drugs, the closest thing to a cure for the “post-starvation syndrome” are presumably leptin receptor agonists.
Though I am biased because of my personal experience.
About a decade ago I dieted down to single digit body fat levels (4.8% at my lowest point) and stayed there for about a year. I did this mostly because of vanity reasons. Back then, my energy levels were abysmal and multiple hormonal axes were in the gutter. My mental health was much worse as well. Even weight regain and starting to eat 3000kcal/d has not fully reversed all of the starvation-related adaptations even years after the fact. The only thing that brought sustainable change was being on low doses of metreleptin for some time. My hypothesis is that being on metreleptin for some time has reversed the hypoleptinemia-induced adaptations on a trophic level. In other words, it changed not just my brain function acutely while I was on it but probably also changed my brain structure, which is known from the literature. There is fMRI evidence that after 1 year on metreleptin, there are a number of trophic changes in brain structure.
I will now lay out what can be done in more detail for people who do not have access to metreleptin because having access to metreleptin is part of the syndrome of the ultra rich.
But first, let’s recap.
In summary, the lack of either calories, insulin, or leptin (all partially independently) signal to hypothalamic “energy neurons” (mostly POMC and AgRP neurons but also others) that there is an energy shortage. These neurons in turn control sympathetic nervous system tone via direct connections to various nuclei in the brain stem. Furthermore, these neurons also co-control all of the major pituitary hormonal axes (HPA, HTA, HPT), and their target hormones (cortisol, testosterone and estradiol, triiodothyronine) have sizeable effects on adrenergic tone (and every other major bodily system).
The combined effect of a direct reduction in SNS activity and a drop in various hormones, produces the syndrome described in the introduction, which is very common among the ultra-fit and chronic dieters. The ultra-fit get there mostly by low leptin levels and the chronic dieters get there mostly by a low caloric intake.
Given that most of the individuals suffering from “sickness fitness” have been living themselves into the condition over long periods of time, POMC/CART neurons need to be “re-taught” that there is plenty of energy available and that there is nothing to worry about. Ultimately, this comes down to increasing caloric intake and gaining adipose tissue – both of which will have independent effects.

Talking to an endocrinologist that researches hypothalamic amenorrhoea in females as well as doing research on former patients with anorexia nervosa myself, it seemed that for some (but not all) a long period of purposeful overfeeding does seem to reverse some -and sometimes even most to all- of the damage. However, most of these “refeeders” do end up being overweight (and some even end up overweight with little to no improvement).
Example: Someone is at 15% body fat while being in good health. For some reason, this person diets down to a body fat to 8% and stays there for a while. For significant recovery to occur the person needs to undergo a period of gross overfeeding and to experience full recovery the person ends up at a body fat above 20% or higher…and this person is then somewhat barred from losing that weight again because that would just start everything over. Some lucky ones recover much more readily it seems.
Super-fit-super-sick syndrome is etiologically similar to what goes wrong in the brains in individuals with anorexia nervosa, just to a lesser extent. Individuals with AN also present with abysmal blood pressure (often in the low 90s) and heart rate (low 40s), crushing fatigue and weakness, sky-high SHBG, and abysmal thyroid and sex hormone levels.
The main (etiological) biochemical abnormality in AN is profound hypoleptinemia and leptin replacement therapy is a currently researched and highly promising avenue to treat it. Unfortunately, pharmaceutical leptin is very hard to get by and it is among the most expensive drugs on the planet – even though it is not more complex to manufacture than insulin. I discuss my personal experience with leptin later.
But let us get to the practical part.
Lifestyle practices do’s and don’t’s
1. No fasting
This one should be obvious. Fasting lowers AUC-insulin and crushes levels of leptin (much more than just the loss of the same amount of fat mass would) -and leptin levels do not really normalize for a long timeafter periods of fasting (regardless of weight regain).
- Fasting is a gateway into eating disorders: Patients with a past eating disorder should not do any fasting because of high relapse potential. During fasting, dopamine amplitude rises sharply. Furthermore, the feeling of accomplishment and the “feeling proud of oneself” is addictive.
- Fasting impairs peripheral thyroid sensitivity (e.g. intracellular T3 conversion)
- Fasting impairs noradrenaline signaling in the long term (explained above)
- Fasting impairs leptin expression in the long term and after short-term fasting leptin synthesis is lower for a long time
- Downregulation in POMC neurons

2. Eating enough calories via reverse dieting
By now it should be evident that there is a whole army of regulatory systems in place that detect caloric flux. It is incredibly difficult if not impossible to outsmart these systems over long periods of time (at least without the injection of multiple peptide proteins – discussed later).
Many people need a lot more calories compared to what TDEE-calculators advocate, esp. if these calories come from real foods which are only absorbed to 80–90% and also need much more energy for their digestion.
Obviously, caloric intake needs to be increased without a concomitant increase in exercise that would burn these extra calories off.
The best strategy I have found is reverse-dieting. Increasing caloric intake by 100kcal per week. In my early twenties, I reverse-dieted my way from 2000kcal to 2500kcal over the course of 5 weeks. Interestingly, I have gained no to minimal amounts of fat but started to feel more vital.
I have seen something similar a number of times – individuals who had been undereating for a long time gradually increase their caloric intake over the span of a couple of weeks. And despite eating e.g., 25% more than before, they gain no to minimal amounts of fat.
3. No low-carb or low-fat
You need both. Carbs are needed to stimulate insulin. Furthermore, the hypothalamus has glucose-sensing neurons, which do feed into POMC-regulatory signals. While low-carbing is okay for sedentary individuals, it is harmful for individuals suffering from super-fit-super-sick syndrome. Fats are needed for CCK release, which acts on the vagus nerve and transmits a powerful satiety signal to the brain. Furthermore, leptin synthesis is dependent on adipocyte fat flux.
Potentially interesting tidbit: I have talked to an endocrinologist specializing in reproductive endocrinology and he told me, that in a special clinic he was working at, they had their patients suffering from hypothalamic amenorrhoea (mostly induced by eating disorders) eat plain old butter, which resulted in some patients spontaneously ovulating. For some reason, butter (or other sources of saturated fats) seemed to be better than other kinds of fats. My hypothesis is that there seems to be something specific about how saturated fats are metabolized in adipocytes. Leptin synthesis in adipocytes is partly dependent on fatty acid and triglyceride turnover, which is low on a low-fat diet and highest in a diet high in saturated fats.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Hacking this ancient system by injecting satiety peptides
Now let’s get to the interesting part.
Given that this blog is primarily about biological interventions there are obviously also pharmacological/hormonal options available to either mimic the signaling of energy abundance or to at least accelerate the whole process of recovery.
Importantly, by pharmacologically “simulating” a period of overfeeding, one may reverse “starvation mode” without the metabolically unhealthy and aesthetically unpleasing fat gain that accompanies the natural route of recovery.
One more time, lets recap what we know:
- There is a specific syndrome that is common in the “ultra-fit”. The same syndrome is found in chronic dieters.
- This syndrome is mostly brought about by the brain perceiving there to be an energy shortage due to insufficient caloric intake, excessive exercise, low body fat levels, or all three.
- Energy availability is signaled to the brain by an army of peptides. Among these are short-terms satiety peptides (GLP-1, CCK, PYY), medium-term (insulin), and long-term signals (leptin).
- The ultra-fit have mostly low levels of leptin, whereas chronic dieters have low levels of other satiety peptides.
- These signals are integrated by a specific group of neurons within the hypothalamus called POMC-neurons, found in the arcuate nucleus of the mediobasal hypothalamus. It seems that periods of starvation (or any proxy of that such as chronic undereating, overexercising, maintaining very low levels of body fat, etc.) somehow “imprint” on the nervous system -presumably in this group of neurons. The most plausible imprinting mechanisms entail either epigenetic changes to key transcription factors or simple synaptic plasticity of the network as a whole.
- If a period of starvation is able to make specific alterations to gene expression and/or bring about a hypofunction in this neural network, then it seems logical that a period of overfeeding may be able to reverse these changes.
- Then, in the same way that a decline in these aforementioned satiety peptides signals the state of starvation, a surplus of these peptides signals a state of abundance.
Well, “this surplus of peptide signals” is certainly something that can be engineered.
GLP-1 agonists
Whereas leptin is the long-acting satiety signal, insulin is the intermediate-acting signal. However, vertebrates also have shorter acting satiety peptides such as CCK and GLP-1.
GLP1 agonists are modified versions of GLP-1 with a much longer half-life – basically sending a satiety 24/7 signal to the brain (very simplistically speaking) by activating POMC/CART neurons.
When I had this syndrome, for me, the introduction of semaglutide into my system eliminated that hard-to-fight urge to constantly eat. The feeling of true satiety, which I had not experienced in a long time, became my new normal state (and I soon got used to it). Before semaglutide, I have not experienced complete satiety for a couple of years and just accepted the constant low-level background hunger. Finally, a normal meal kept me satiated. I got still hungry if I did not eat but the “ravenous” hunger was gone.
Furthermore, my resting heart rate rose from the low 40s to the low 50s. My energy levels increased. My TSH, LH, FSH, testosterone, and estradiol all rose to normal levels within 3 weeks of starting semaglutide.
Also, within a week or two, I noticed that I sweat much more and much more easily and that the heat intolerance, which I had been plagued with for a long time, was gone (partially because I had a hard time sweating before). This also, is an indicator that my sympathetic nervous system picked up.
Semaglutide also eliminated this weird distinct “feeling like shit”, which in the past could be eliminated only by taking cortisol (or ingesting/doing something that raises cortisol such as exercise).
Initially, I lost some weight (which I purposely tried not to), but as my body fat approached single digits, the feeling of hunger and weakness returned. Even though a small meal would now satiate me quite quickly, I nonetheless got hungry quite soon after eating. Self-experiments with metreleptin have shown me that this was due to low leptin levels (discussed later).
Ultimately, semaglutide helped but was not a “cure”. While I mostly felt normal, I could still feel that some things were “off”. My energy levels and mood were definitely not back to normal levels and I was much less “bubbly” than I normally am. The two biggest downsides of semaglutide were:
- Semaglutide caused slight anhedonia.
- Semaglutide made it almost impossible to gain weight, which prevents the necessary rise in leptin levels (remember: leptin is more powerful than short-term satiety peptides acting on G-protein coupled receptors).
I discuss my experience with semaglutide in more detail here.
Insulin
Despite of what all the “influencers” in the sphere are preaching, insulin is not exclusively bad. Sure, it drives the mTOR pathway (and therefore aging) and hyperinsulinemia is associated with all kinds of chronic diseases, such as cancer, dementia, and atherosclerosis.
But as so often, the dose makes the poison. Insulin is similar to insulin-like-growth factor 1 (IGF-1). Both of these are anabolic hormones, perhaps the most anabolic hormones known to mankind. Insulin is also responsible for driving glucose and amino acid into cells, inducing them to be active.
Furthermore, and most relevant to this article, insulin is a powerful medium-term satiety peptide, and gives a “go-ahead” signal to the hypothalamus that the organism has plenty of resources to use for activities besides acquiring food. This is part of the reason many women start to lose their period when they switch to keto or intermittent fasting – even if they do not lose any weight.
What is more, cumulative effects of insulin have trophic effects on POMC neurons, as insulin acts on a receptor tyrosine kinase inducing POMC neuron hypertrophy.
Insulin also stimulates leptin synthesis. Furthermore, insulin stimulates hypothalamic release of hormones. Moreover, it stimulates the conversion of T4 →T3. In addition, insulin stimulates IGF1-synthesis. Insulin also lowers the synthesis of hormone binding proteins (e.g. SHBG, TBG, CBG), which causes a slight uptick in equilibrium of free vs. bound hormones. All of this helps with energy levels and vitality.
When “the hormone of abundance” is very low, such as in type I diabetes, individuals basically “wither away”, both mentally and physically – in part because their cells stop metabolizing nutrients and enter a kind of “conserve resources mode”.
While we certainly want to have AUC-insulin on the lower end for longevity purposes, for the purpose of repairing our metabolism we do want to keep insulin levels fairly high, or at least normal, for some time.
Many people with already “starved” metabolisms throw in intermittent fasting or a keto diet, which exacerbates the starvation response, as the cumulative effect of insulin on POMC neurons are now lacking.
Insulin is “the hormone of abundance” and as such, it is one of the main signal conveying to POMC neurons that we are in an environment where food is plentiful.
A normal physiological production of insulin is about 60 IU per day. Of this, 30 IU are as a basal insulin (constantly trickled into the blood stream) and roughly 30 IU in response to eating food (prandial production of insulin).
So, what would happen if I, say, add 5 IU of a long-acting insulin to my physiology? Presumably not much because that would only slightly elevate my total insulin.
Wrong. When I had this syndrome, even a low amount of insulin significantly increased my energy levels and mood. And the change in how I felt was quite striking. Furthermore, my heart rate variability (as measured by my Oura ring) decreased by about 10 points and my resting heart rate at night increased by 5 points (from about 45bpm to about 50bpm).
All of these changes are indicators that my sympathetic nervous system activity increased. After 10 days, I then stopped the insulin injections and on that day I felt tired, “weak” and moving around was particularly onerous. The changes in resting heart rate and HRV reversed – indicating that my sympathetic nervous system output had dropped again.
I also got lightheaded multiple times, presumably because my CNS had partially adapted to the higher SNS-activity, analogous to how people feel tired and weak after having taken simulants for a couple of days and then suddenly stopping. I then reintroduced 5 IU of insulin degludec and lo and behold, my SNS activity rose again.
I repeated this experiment a year later. Same response.
From this I learned that my basal insulin levels were very low – perhaps too low. In fact, whenever I measure my fasting insulin or C-peptide (a peptide co-secreted with insulin), the results always come back below the reference range. For longevity purposes, this is great. However, for vitality purposes not so much. As so often, vitality and longevity are at odds.
Just as semaglutide (plasma half life of 5-7 days) is a long-acting modification of GLP-1 (plasma half-life of about 5 minutes), the same holds for a long-acting modifications of insulin (which normally has a half-life of about 5 minutes as well). Thus, the long-acting insulin continues to constantly act on POMC neurons throughout the day.
When I eat a lot of carbs or animal protein, insulin levels rise for some time, and then they fall again. However, basal insulin levels do not change and for very insulin-sensitive individuals such as myself, it may make sense to increase basal levels of insulin for some time which can only be accomplished with long-acting insulins.
Of note, insulin degludec had more pronounced effects than insulin glargine or insulin detemir – 3 different forms of long-acting insulins that differ in their half-lives and presumably also in their ability to cross the blood brain barrier.
I tried this experiment twice, separated by about 2 years. Both times, after one month, I noticed that my hair (arms, chest, beard) grew decently faster.
Given that diabetics inject up to 50 IU of insulin per day for decades I deem up to 10 IU of additional basal insulin per day for a few months to be of negligible risk. Nonetheless, after a month or so, I came off the insulin but decided to change my diet in a way to elevates insulin levels. For example, I started to incorporate more dairy products (which I respond well to), more carbs, and more unhealthy foods in general.
I discuss insulin in more detail here.
Leptin
Leptin is certainly the most powerful of the interventions discussed thus far – by a large margin. And probably more powerful than all the other interventions thus far discussed combined – because it is causal.
While GLP-1 agonists are “a poor man´s leptin”, as in some effects of leptin can be copied (but not others), real leptin is the real deal. While GLP-1 agonists work amazingly in obesity (but leptin receptor analogs not), GLP-1 agonists work poorly/incompletely in super-fit-syndrome but leptin works perfectly well.
The first time I tried leptin was magical. Unexpectedly, I felt the leptin already 2-3 hours after my first injection.
Unfortunately, metreleptin is hard to impossible to get hold of. To me it seems that synthetic leptin can help myriads of fitness-obsessed individuals in quite a life-changing way. And leptin analogs are probably the only molecules that can give people the best of both worlds (i.e., remaining at low levels of body fat while feeling and functioning normally).
I discuss my experience with metreleptin coarsely here but I am planning on writing a much more in-depth article on the subject: My Experience with Leptin
Sign up to my newsletter to get notified when the in-depth article is available
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Without leptin analogs, as a member of Homo sapiens, we have to accept that body fat levels must not be lower than our genetic set point, and there is no way to circumvent this – at least if vitality and mental sanity are a priority. Many have learned the hard way.
Chimps can get away with it (because evolutionarily body fat was never that important) but we do not.

The primary (biological) problem with the super-fit-super-sick-syndrome lies high-up in the nervous system and has been mostly brought about by long-standing hypoleptinemia (I say mostly because there are other minor factors at play) and can also be mostly cured by leptin administration.
Leptin administration not only normalizes sympathetic nervous system function and hormone levels but also helps with the more “mental” aspects of this syndrome, such as rigidity and neuroticism.
Bonus article: Energy Metabolism (Technical Article)
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.