
Many of us want better energy, mood, motivation, sleep, concentration, looks, and health. All the focus is on pharmaceutical drugs, diet, sleep, exercise, gut health, and supplements. For a long time, neither laypeople nor doctors gave hormones the credit they deserve. That seems to be changing now.
In my early twenties, my life was going down the gutter and started to fall apart in every domain. I found out that multiple of my hormones were low. I started to replace what was missing, and my life got back on track. As I experienced for myself: if you change a hormone, you change a life.
Why hormones are neglected by mainstream medicine the way they are is beyond me. Hormones affect everything. By affecting many different organs, tissues, and countless other signaling molecules, they have a powerful influence on systemic health indirectly. By having a major impact on our energy levels, mood, and well-being, they have a mighty say in the lifestyle we lead, which has a major effect on health by itself (most of our modern, chronic diseases are to a large extent lifestyle-induced).
Given their importance, it is worth giving a short, unconventional introduction to these molecules that are pulling the strings in the background all life long.
How hormones came to be
Basic bio intro. Life consists of cells. Cells are biological machines emerging from the laws of chemistry and physics. Cells just do what they are programmed to. The blueprint for this program is written in the form of DNA, the genetic code.
A multicellular organism relies on many different functions carried out by its many different specialized cells. Each cell contributes to, and benefits from, this homeostasis. In multicellular organisms, there are signaling molecules that tell these different cells how to behave. These molecules used for intercellular communication we call “hormones”.
Multicellular life evolved many times independently. Multiple times in single-celled organisms (bacteria and archaea), and many times in protists (single celled-eucaryotes). The latter gave rise to the multicellular kingdoms of life most of us are familiar with because we can see them without a microscope: fungi, plants, and animals.
Around a billion years ago or so, these multicellular “organisms” were not the way they are today. In fact, they were not a single “organism” but rather a sort of biofilm (a collection of individual cells held together by a common structure).
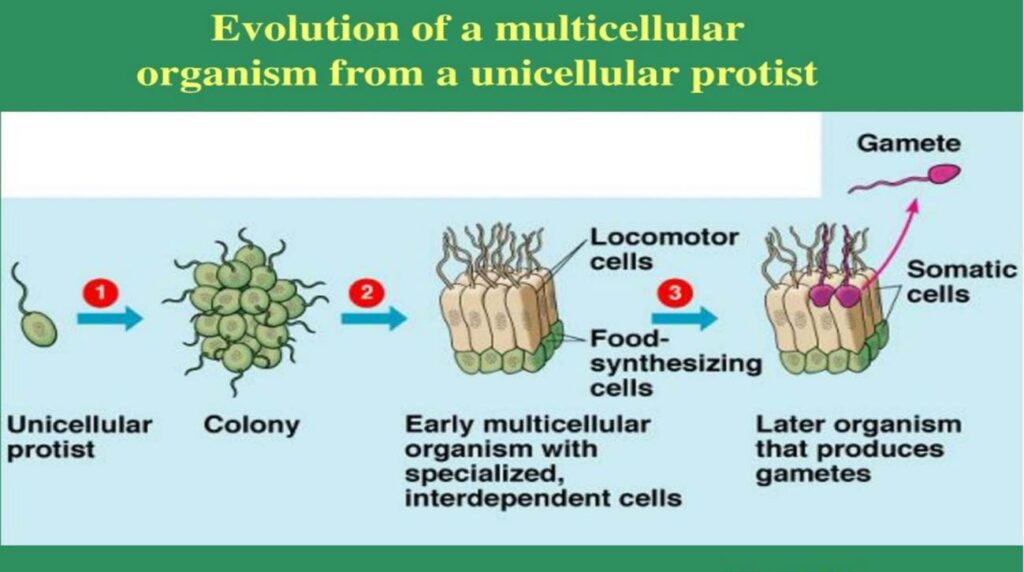
The cells in these biofilms cooperate to ensure the survival and propagation of the cell colony. They work together to effectively make more of themselves (survival + reproduction), which is the point of life from a biological perspective. To do this more effectively and efficiently, these cells perform some division of labor and specialize in different tasks such as defense, feeding, and reproduction.
As these biofilms became more complex and coordinated, two types of molecules became critical:
- Adhesion molecules. Proteins, carbohydrates, or lipids evolved to hold together this uncoordinated mass of cells and prevent it from falling apart.
- Signaling molecules. Proteins, carbohydrates, or lipids were harnessed not just to ensure structural integrity, but also to exchange information between cells. These molecules were used to send, and receive, information about what to do and how to behave.
Cells used these signaling molecules to instruct each other on how to behave under certain circumstances in order to serve the greater good. For example, they were used to tell other cells whether to grow, stop growing, invest in defense, migrate to a different part of the “body”, and even what type of cell to become (specializing in feeding, defense, reproduction, structure, etc.).
In the same way these signaling molecules (mediators) ever since coordinated the behavior of individual cells in those tiny, primitive organisms, they now orchestrate the many different cells in our enormous, ultra-complex, fascinating, vertebrate bodies.
Hormones are signaling molecules. They are used to tell a cell how to behave.
Cell-cell communication is crucial in multicellular organisms. There are hundreds of different signaling molecules in our bodies. Many act mostly locally (e.g., prostaglandins, some cytokines, purines), regulating our cells’ local environment in the sub-millimeter range. The local molecules we do not call hormones but rather “paracrine mediators”.
However, if a signaling molecule is used to coordinate many different cells at a supra-tissue scale (i.e., affecting countless cells or even the whole organism at once, generally using the bloodstream as their highway), we call this mediator a “hormone”. In other words, we call a signaling molecule a hormone if the bloodstream (vs. the interstitial fluid) is used for its transmission between cells. However, there are also intermediate molecules – nature does not care about our names and labels.
The whole point of hormones is to tell different cells at different parts of a multicellular organism how to behave.
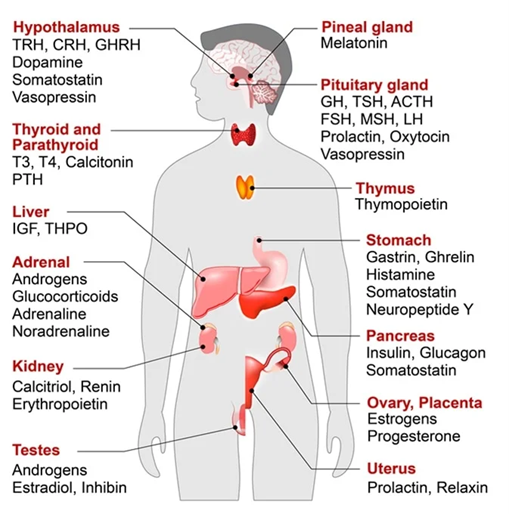
In the human body, there are several dozen systemic hormones. “Systemic” means these molecules are capable of reaching every single cell in the organism by being secreted into the bloodstream. These hormones then “talk” to every cell that has a receptor for them. By extension, each cell can only respond to the hormones it has receptors for.
Many of these systemic hormones serve very specialized purposes, and just specialized cells have receptors for them. For example, vasopressin mostly acts on blood vessels to constrict, and instructs certain cells in the kidney to reabsorb water. Parathyroid hormone mostly acts on cells involved in calcium metabolism. GI peptides mostly act on the cells involved in appetite regulation and nutrient metabolism. Many of these hormones are quite unknown and most people have no interest in reading about, because for most practical purposes they are irrelevant. Some of these hormones include adipokines, myokines, and cytokines. If all of these are included, then the list of hormone-like signaling molecules approaches well over a hundred. However, they vastly differ in their importance. Some of them are quite redundant and therefore somewhat expendable and knockout studies often show no discernible phenotype.
Of note, fast and targeted signals are generally sent via specific nerve fibers to a specific target organ or tissue (using neurotransmitters as messengers). Whereas neurotransmission sends signals in a “cable-like manner” directly to a distinct location to change the activity of the innervated cells (usually only for very short timespans), hormones act systemically throughout the cell colony to coordinate the behavior of all cells. Many of these hormones sent via the bloodstream affect the behavior of the target cell for minutes to hours.
The Big Four Hypothalamic Axes
If my body is a country, then the master government is the hypothalamus.
In vertebrates, it evolved that the major hormones are regulated in a cluster of neural networks called the hypothalamus. The hypothalamus is basically the government of my cell colony.
The hypothalamus is the main interface between the brain and the body. It can be summarized with one word: homeostasis. It regulates temperature, osmolarity, concentration of nutrients, circadian rhythm, the big four hormonal axes, and some other things. Importantly and often neglected, the hypothalamus also regulates our three most important drives: eat, sleep, fuck, repeat. Some also include fighting in this. Eating to maintain nutrient and energy homeostasis, sleeping to maintain brain homeostasis, fucking to maintain homeostasis as to the number of individuals in a species, and fighting to maintain territorial or bodily integrity. Most vertebrate animals, including humans, spend large chunks of their time on these behaviors.
There are 4 types of hormones everyone should know about. They are all regulated by our hypothalamus. These we call the big four hypothalamic axes. Each has a profound influence on every single cell in our body, and thus on us as an organism as a whole.
These are also the hormones that most likely come to mind when you think of “hormones”. Each serves a specific function:
- Growth hormones regulate cellular growth and maintenance. The hypothalamus secretes GHRH -> growth hormone (GH) -> the liver secretes IGF-1, which is the primary growth factor in the vertebrate body.
- Sex hormones regulate all things concerning reproduction. The hypothalamus secretes GnRH -> LH & FSH -> the gonads respond with the secretion of sex hormones, of which the major ones are testosterone, estradiol, and progesterone.
- Stress hormones prepare the body and brain for action. The hypothalamus secretes CRH -> ACTH -> the adrenal gland secretes cortisol.
- Thyroid hormones determine how fast metabolism goes, and therefore how much energy we use. The hypothalamus secretes TRH -> TSH -> the thyroid gland responds with the secretion of thyroxine, T4, and its more active form tri-iodothyronine, T3.
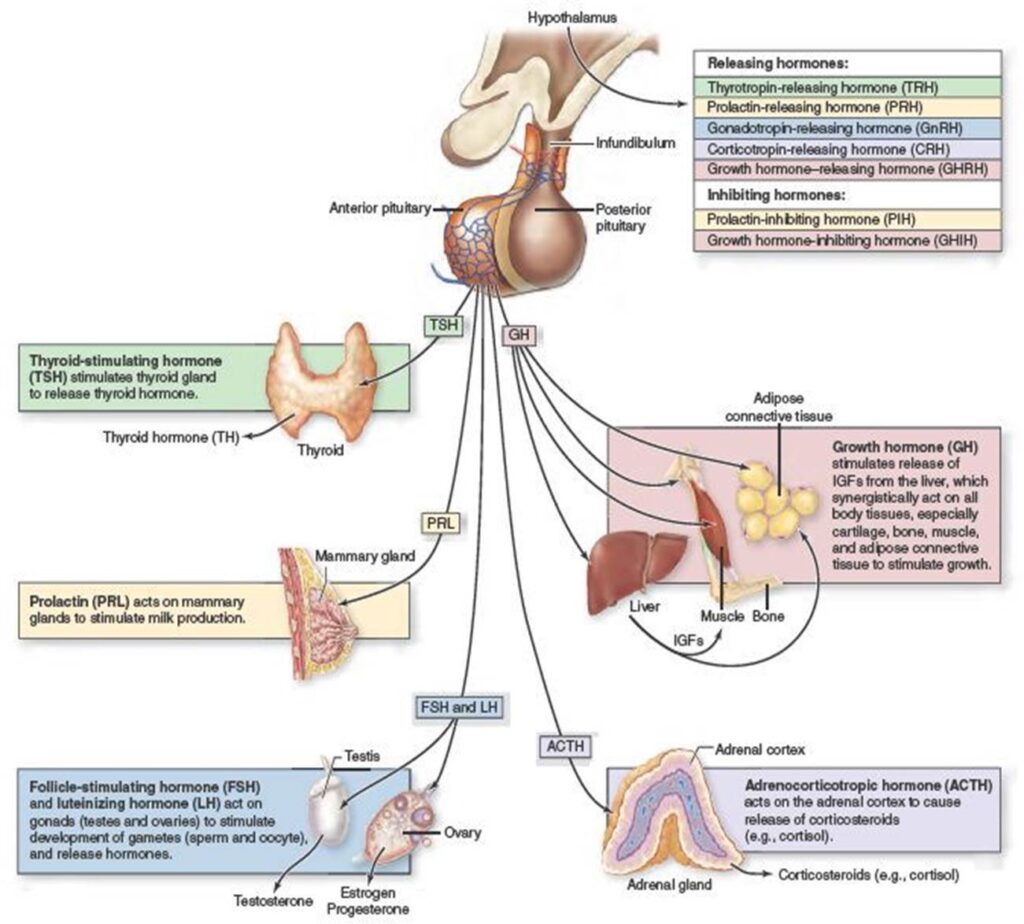
The major endocrine axes in our bodies are all regulated by the hypothalamus.
This central regulation allows the whole organism to respond in a coordinated manner by a single whole-body signal. These slow whole-body signals are transmitted via the bloodstream, using hormones as messengers.
In contrast to most other hormones, every single cell in our body has receptors for all four types of these hypothalamic hormones. And with the exception of IGF-1, they each directly unlock a specific portion of the genetic code, depending on what part of the code is accessible in that tissue. By acting at the level of this code directly, these hypothalamic hormones are one of the main factors that determine which programs are running in any given cell at any given point in time. Therefore, in a way, these can be considered the most important and most powerful hormones in your body.
Technically, prolactin is also an anterior hypothalamic hormone but its importance is debated and I am neglecting it for practical purposes.
Articles:
- Thyroid hormones
- Testosterone (TRT)
- My TRT Lite Protocol
- Cortisol
- Other hormones (GH, Insulin, EPO, Estrogel, Oxandrolone, Oxytocin, etc.)
- Leptin – The Most Expensive Hormone on Earth
Why the Big Four hit different: receptor mechanics
This part is getting a little technical, but bear with me. Understanding the following points is crucial to understanding the true power of hormones.
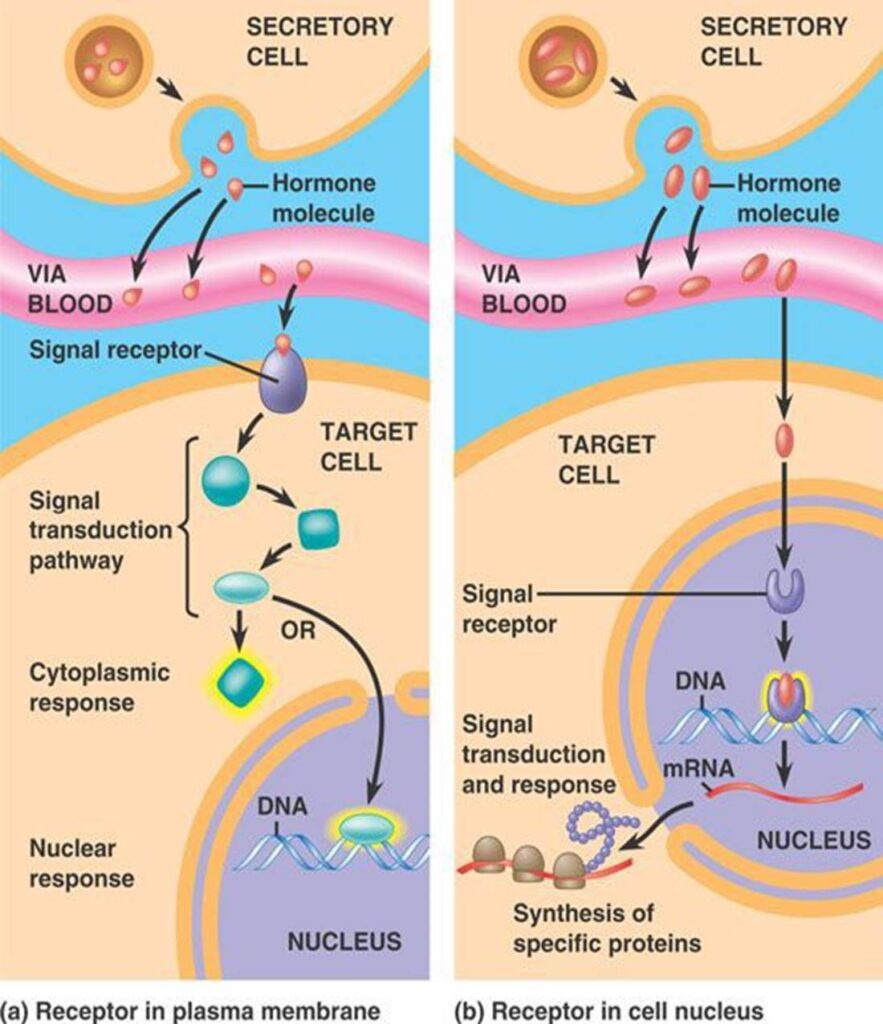
There is a fundamental difference between the many systemic hormones and the target hormones of the thyroid axis (T4, T3), reproductive axis (testosterone, estradiol, progesterone), and stress axis (cortisol). The difference is in how our cells respond. And how a cell responds depends exclusively on the type of hormone receptor.
In general, we subdivide hormone receptors into two categories.
1. Transmembrane receptors: fast, mostly transient
Most signaling molecules in our bodies act on transmembrane receptors. They lead to an immediate change in our cells’ activity (seconds), some activity changes (minutes), and also some minor gene expression changes (hours to days). Whenever the receptor is activated, it tells a cell to “work harder” (e.g., brain cells), to “contract” (e.g., muscle cells), or to “release whatever they have stored” (e.g., endocrine cells). For practical purposes, I am neglecting the effects chronic over -or underactivation of certain signaling pathways have on gene expression.
Many of the pharmaceutical drugs we use in medicine act on these membrane receptors.
For example, adrenaline acts on many different cells throughout your body to change their activity so they can better respond to danger (liver cells breaking down glycogen, cells in the airways relaxing, blood vessels constricting in the skin but widening in the muscles, changes in neural processing, etc.).
2. Nuclear receptors: slow, persistent
Hypothalamic hormones (other than IGF-1) are different. These hormones do not act on receptors on the cell membrane. They act on nuclear receptors.
Getting a little technical again. The identity of every one of our cells (for example, a muscle cell being a muscle cell) and the activity of every cell (for example, a muscle cell contracting) depends on which genes a given cell expresses, which is set up during early embryonic development.
What genes a cell expresses is determined by a combination of, firstly, gene methylation (which turns a gene down or even off), and secondly, specific transcription factors (which can turn a gene up or down). Given a gene is not methylated, a combination of specific transcription factors determines how much, and under what circumstances, a gene is expressed.
During embryogenesis, the same molecules that run our adult bodies were also used to instruct cells on what type of cell to become. Local and systemic hormones precisely regulated how you developed from a single fertilized cell into the elaborate 3D cell colony you are now. They told your cells both how to behave and what to become. For example, liver cells performing most of the metabolism for the cell colony and supplementing what other cells might need, lymphocytes being there to recognize intruders and to assassinate them, skin cells sacrificing themselves to form a mechanical barrier consisting of hard dead cells, ameloblasts building enamel for your teeth’s outer surface, and germ cells being there to propagate your genetic material into the next generation.
Development is a program in which a three-dimensional collection of cells shapes itself over time by a cascade of highly regulated and beautifully orchestrated sequential inductions of genes. It blows my mind that such an incredibly elaborate cell colony like our body, with all its insanely intricate subsystems such as the immune system, the nervous system, the sense organs, can be crafted by the same single genome, with just around 20.000 pieces to the puzzle. 20.000 potential “weapons” a cancerous cell can use to turn against the cell colony by unlocking functions that should be off the hook for it. These genes are precisely regulated regarding both time and location of their expression.
No wonder Alan Turing was deeply fascinated by embryology. He could not wrap his mind around the fact that so much information can be packed into a single genome, determining both the micro-universe of a single cell, and the even more incredible structural and functional orchestration of the whole cell colony, all at the same time, giving rise to this beautiful body of ours. What is breathtaking is the genetic programs behind even elementary things we take for granted. A specific tooth erupting at a specific time, shaping itself into a form slightly but distinctly different from its neighboring teeth. The branching geometry of a lung. The mosaic of cone subtypes in the retina. Everything coded for by a single genome. The more you learn, the harder it is to believe any of this is physically possible.
Anyway, the genes that have not been turned off permanently (e.g., genes only useful for immune function will be turned off in most of our non-immune cells quite early in embryonic development) can be turned up or down throughout life. Whenever a gene is turned up (after a transcription factor binds to the gene’s promoter), the cell expresses more of the gene product (a certain protein). When a gene is turned down, the cell expresses less of it.
The kind and the amounts of certain proteins in any given cell constitute its inner machinery, which determines both a cell’s identity (e.g., muscle cell) and behavior (e.g., contracting).
Determination of a cell’s identity is mostly complete before birth. In an adult organism, any given cell just has a limited number of genes it can still express (around one-third to one-half of the genes will have been turned off permanently). Therefore, major identity changes are not possible anymore (other than in stem cells). However, if we change the kinds or amounts of the proteins that are still available for gene expression, the cell still changes its machinery, which also changes its behavior.
The whole point of signaling molecules is to send messages to other cells to instruct them on how to behave. If these messages change, then so does the behavior of the cells that receive them.
If nuclear receptors are activated, they lead to a change in certain proteins’ amount, but not their activity (for most practical purposes) . The effects are not visible for at least 30 minutes or so, and they are gradual, unlike the “bam” effect from the activation of membrane receptors. However, once the cell has changed its internal machinery, the effects last as long as these proteins exist in the cell, generally from hours to weeks.
Thyroid, stress, and sex hormones all act on these nuclear receptors. This means they instruct our cells to change the kinds and amounts of certain genes, which leads to a change in the kinds and amounts of certain proteins, which then leads to a change in the cell’s internal machinery. The change lasts as long as these proteins are not degraded.
What is unique for the hypothalamic hormones is that every single cell in your body has a receptor for them. So if we change any of these hormones (contraceptive pill, stress, bodybuilder injecting testosterone), we are talking directly to all of your cells at once. Every single cell in the body changes its machinery, in a dose-dependent fashion. (Of course, the exception is cells that have no nucleus, such as red blood cells.)
Of note: In addition to nuclear receptors, membrane receptors for almost all of these hormones have been identified (e.g., mGR for cortisol). While they do have an effect and serve a purpose, not much would happen if you did not have these membrane receptors. In general, almost everything in the body is redundant to some degree.
A worked example: the contraceptive pill
If a woman takes an oral contraceptive, she is ingesting a synthetic version of estradiol (usually ethinyl estradiol). The molecules are absorbed into her bloodstream and travel to all of the body’s cells. There they diffuse through the cell membrane and bind to the nuclear receptor for estradiol (the estrogen receptor, or ER).
The ER then translocates into the cell’s nucleus, where DNA is floating around. There, the ER binds to hundreds of genes that have a certain estrogen-response element in the sequence of the gene’s promoter. Now the cell turns up the expression of these genes, which are mostly genes necessary for female reproduction.
For example, cells in the liver start ramping up the production of proteins that otherwise would occur during pregnancy. Cells in the lining of her uterus are told to grow and proliferate in order to prepare for implantation of an embryo (which is why estrogens are said to promote the advent of uterine cancers). The immune cells slightly change their behavior toward one that is more suitable for pregnancy. Cells in the skin increase blood flow and become warm and moist. Hair cells are stimulated to grow, and her hair grows lusher as an indicator for sexual signaling. In many other species, female genitals become engorged with blood to signal sexual receptivity to males.
Of course, estradiol also has many specific effects on brain cells. Emotionality, motivation, mood, and cognition all change in a way suitable for reproductive purposes. (With testosterone administration in males, there would be an increase in alertness, drive, and libido.) Thousands of other changes throughout the body prepare the whole organism for reproduction, not just structurally and functionally, but also behaviorally.
This whole-body regulation of these major hormones also shows how big of a intervention e.g., TRT is. Modulation of androgen and estrogen receptors changes the expression of hundreds of genes.
Hormones change if conditions change
For all of these hypothalamic hormones, we have a certain setpoint. The setpoint determines how much of a given hormone should be present at any given time. If hormone levels are lower than that (or the setpoint adjusts upwards), the respective hormonal axis is upregulated. If hormone levels are higher than that (or the setpoint adjusts downwards), the hormonal axis is downregulated.
However, this setpoint is quite plastic and can be shifted upwards (e.g., the cortisol axis before awakening) or downwards (e.g., the thyroid axis whenever we are fasting) depending on various internal and external conditions. The whole purpose of constantly changing and adapting these setpoints is to coordinate the behavior of all of the cells in our organism so that we, as an organism, are better able to cope with a given set of conditions (time of day, food abundance, season, stress).
For example, let us say we experience any sort of trauma, physical or psychological. This input reaches the hypothalamus via nerve fibers, which causes the hypothalamus to react with appropriate hormonal changes (in this case, an increase in the setpoint of stress hormones, to prepare the organism for action). Among other things, adipocytes start to break down and release fatty acids. The liver makes new glucose and also breaks down stored glycogen to be used by the heart, muscle, and brain. The nervous system increases its readiness (alertness sharpens, executive functions are upregulated, memory formation is stimulated). At the same time, nonessential functions such as digestion or reproduction are downregulated as long as these signals (and therefore high levels of cortisol) are present. In fact, stress hormones directly or indirectly alter the expression of about 20% of all our genes. A similar effect can be seen with the other three hypothalamic axes.
How are these setpoints determined?
To determine the appropriate hormonal setpoint for a specific set of conditions, specific neural networks within our hypothalamus integrate many different kinds of inputs. Inputs come from our blood (hormone levels, nutrients) and from our brain (sensory input, thoughts). After integrating all this information, these networks “decide” on a specific setpoint (e.g., a setpoint for free testosterone at 18 ng/ml, equating to a specific activation of the androgen receptor and the estrogen receptors). These networks try to match the blood hormone levels they are non-stop monitoring to the setpoint’s setting.
If hormone levels are lower than that, they send signals to the peripheral glands to instruct them to produce and release more of the target hormone into the bloodstream. Via the bloodstream, this hormone reaches every cell of our body, instructing it to change its interior machinery and therefore behavior. Furthermore, it also reaches these hypothalamic networks, which continuously compare blood levels to the setpoint for a given hormone.
For example, if a male is surrounded by horny and pretty females, the setpoint for he sex axis will be upregulated. Similarly, the perception of winning (vs. losing) in life also seems to upregulate the sex steroid setpoint.
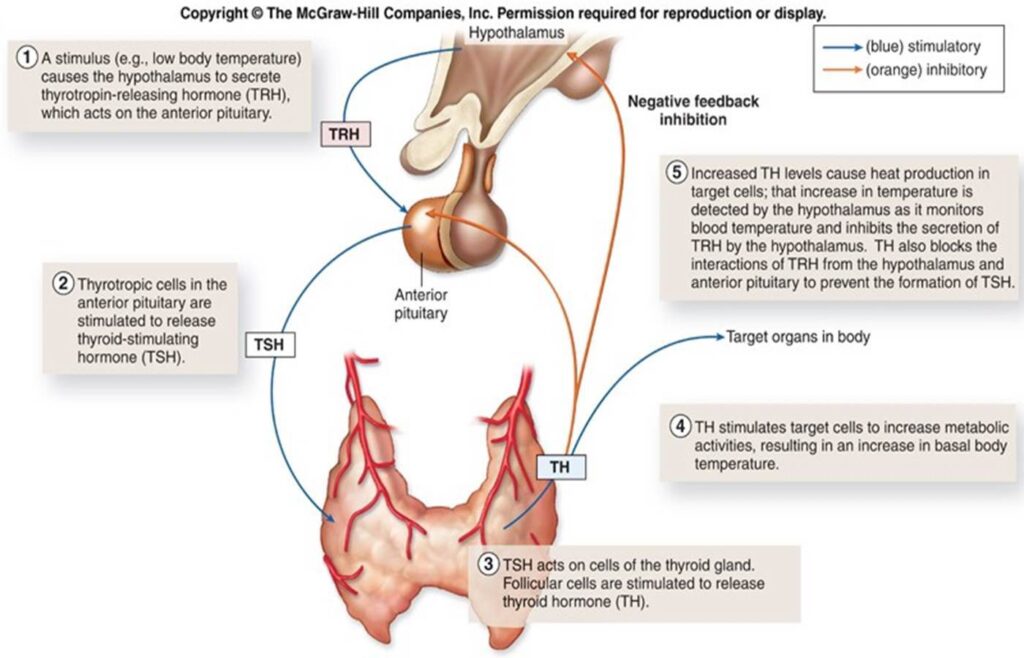
An example of how the thyroid axis works. Low body temperature (top left) acts as a stimulus for setpoint change.
To relate to the picture above: let us say we deprive ourselves of calories. Due to various convergent inputs reaching the hypothalamus (a drop in insulin and leptin, a drop in body temperature), the setpoints of our thyroid and sex hormones are shifted downwards, while the setpoint for stress hormones is shifted upwards. These hormonal changes then affect every single cell in our body in a specific way (and therefore every tissue, organ, and organ system), to be better able to cope with the conditions of food deprivation. Among other things, this coordinated hormonal response leads to a slowdown of metabolism, a shutting down of reproduction, the liberation of fatty acids, and stimulation of hepatic gluconeogenesis.
Alternatively, if we increase our caloric intake, especially carbohydrates, our hypothalamus will increase the setpoint of our thyroid hormones because “Hey, there is enough energy now. Use it!”. The setpoint of our thyroid hormones determines how fast things are happening. If things are happening faster, our cells burn through more energy (our basal metabolic rate is now higher, and we automatically burn more calories doing nothing).
Why should you even care?
The hypothalamus can be seen as the cell colony’s government. It tells all of our cells in a coordinated manner how they should behave in order to serve the greater good. If things are suboptimal and/or go wrong with our hormones, our bodies and minds will follow.
On the other hand, if we mess with any hormone (contraceptive pills, replacing thyroid hormones, TRT), we bypass our cell colony’s government and are directly “talking” to every single cell in our body. It is now us that is sending whole-body messages to all of our cells and therefore telling them how to behave. This is far more powerful (+/-) than taking a drug that affects a single target.
Bypassing our cell colony’s government by exogenous replacement of hormones is not necessarily a bad thing, because the way this government evolved to regulate our organism (what signals it uses to determine the “appropriate” hormonal balance) is adapted to different times and conditions. Times and conditions that are very unlike the modern world. It is not adapted to an overabundance of food, intense blue light at unnatural times, constant low-level stress, or fast-spiking carbohydrates. It is adapted to times when primates were climbing in trees, or when early hominids were browsing the African grasslands. A world completely different from our own. So we could argue that living in today’s world is just as “unnatural” as interfering with our cell colony’s government.
If we change a hormone, we change our body, mind, and life. Thus, the right or wrong choice has potentially life-changing consequences, in both directions (career, fertility, health, mental health).
Part II – The Life-changing Power of Hormones
I find that life is much easier and much more enjoyable if I have great energy levels, mood, and health. In fact, whatever I want in life, great vitality is perhaps the most important requirement to get me there.
As it turns out, my vitality is closely dependent on my hormonal balance. If even one of my major hormones is off, my vitality takes a severe hit, and no lifestyle intervention, supplement, or drug can remedy that.
Conversely, I was more vital, energetic, and emotional during puberty, a time during which most of my major hormones were at their peak, and there is in part a causal connection.

Many of the major hormones affect every bodily system because they modulate cellular gene expression directly – the deepest and most powerful layer of intervention.
My experiments and experiences with hormone replacement lead me to believe that a non-minor subset of people who have to rely on stimulants to function and be productive may simply have low levels of testosterone, cortisol, thyroid hormones, leptin, or a combination of these.
Experience reports for individual hormones:
Some general stuff about hormones
Life consists of cells. Cells are biological machines emerging from the laws of chemistry and physics and just do what they are programmed to. The blueprint for this program is written in the form of the genetic code.

A multicellular organism relies on the different functions carried out by its many different specialized cells and each cell contributes to and benefits from homeostasis, whose ultimate point is survival and reproduction of the organism. For the coordinated function of these many different cells, systemic coordination is necessary.
Multicellular organisms evolved signaling molecules to coordinate the activity and behavior of the different cells separated by a distance. Next to local small-scale coordination via paracrine mediators, there are certain signaling molecules that are used for large-scale coordination of many different cells, tissues, and organs at the same time. These systemic signaling molecules are called hormones.
Some of the major hormones, including steroid hormones (e.g., cortisol, estradiol, testosterone), thyroid hormones, and IGF-1 act on pretty much every cell of the body at the same time. By acting on the blueprint written in the form of the genetic code, these hormones instruct cells on a body-wide level how they should behave.
For example, insulin signals to store nutrients and regulates metabolic flux, thyroid hormones determine the metabolic rate, sex hormones instruct the organism to get ready for reproduction, IGF-1 induces growth and repair, cortisol instructs cells to prepare for stress, etc.
Many of the major hormones achieve this systemic coordination by directly affecting gene expression (among other things) and are therefore among the determinants of what programs -and to what extent- are running in any given cell at any given point in time.
With very few exceptions, almost every single cell in the human body has millions of receptors for all of the major hypothalamic hormones (sex hormones, stress hormones, growth hormone, thyroid hormones).
Each of them unlocks a specific portion of the genetic code, depending on what part of the code is accessible, which differs between tissues. This is what makes hormones uniquely powerful – far more powerful than a pharmaceutical drug merely affecting a single target.

Each of the major hormones affects each single cell in multiple ways.
- Firstly, as explained above, many hormones have direct genomic effects that alter the expression of the genetic code, sometimes in major ways. For example, testosterone causes the expression of hundreds of genes that have the androgen response element in their promoter region. The expressed proteins then alter cellular function in testosterone-specific ways, such as hypertrophy in muscle cells, maturation in sperm cells, or an increase in the activity of dopamine-producing neurons.
- Secondly, hormones have indirect effects because each hormone affects many other hormones and mediators. For example, testosterone affects levels of cortisol, insulin, leptin, oxytocin, and IGF-1, which each then have effects on their own.
- Thirdly, hormones affect energy levels, mood, and health and therefore have a major influence on behavior, which then affects the lifestyle choices people make, which then affects the whole body in a number of ways. For example, testosterone increases energy levels, motivation, and stimulates musculoskeletal changes, which then affect the desire and ability to exercise.
As may be evident by now, if one of the major hormones is off, this will have major effects on the whole organism, ranging from genome, cell, tissue, organ, physiology, behavior, and life situation. Conversely, hormone therapy is perhaps among the most holistic therapies currently available – holistic in the sense of affecting all aspects of the body and mind.
While the mechanism of action of most pharmaceutical drugs is usually high upstream in the signaling hierarchy, many hormones act at the most downstream level possible (gene expression) affecting the whole organism from deep within. Each of the major hormones modulates every bodily system, having powerful effects on the cardiovascular system, immune system, musculoskeletal system, liver, kidneys, brain, etc.
In my opinion, using these natural molecules my body had been adapted to for millions of years is more “natural” and more effective (and presumably also healthier) than the current medical practice of sick care (instead of health care) to prescribe a cocktail of different drugs to patch up all the individual symptoms, complaints, and every abnormal physical or laboratory finding separately.
For example, hypothyroidism is associated with fatigue, depression, weight gain, and dyslipidemia. Often, these symptoms are patched up individually with caffeine, antidepressants, metabolic drugs, and lipid-lowering agents.
Why are hormones underused?
Diet, exercise, sleep, stress reduction, and connection with others are all important for living a long and healthy life. But few things have as profound an immediate impact as restoring hormones to optimal levels.
Unfortunately, hormones are something doctors rarely properly look at, and hormone replacement therapy is rarely used by most doctors. In fact, many doctors are scared of it. In my experience, most doctors would rather prescribe a cocktail of unnatural drugs instead of the necessary bio-identical molecules. I suspect that this is mostly industry-driven.
Speculatively, hormones are widely neglected by mainstream medicine in part because the evidence for these natural molecules is quite poor (however, absence of evidence is not evidence of absence). The medical system is a huge industry and as is the case with other industries, it depends on revenue generation (“follow the money”).
Most revenue is made from patents. However, hormones are natural molecules, which nobody is allowed to patent. Therefore, since not much money can be made from hormones, they do not have as much evidence behind them as pharmaceutical drugs, given that a lot of evidence generation is funded because of financial incentives.
The evidence-generation process is a revenue-generation process, distorting medical science so much that many physicians have unfounded confidence in unnatural drugs while remaining ignorant and fearful of natural hormones.
Even though not (yet?) widespread, the use of hormone therapy is no secret, and many doctors around the world have recognized their unparalleled power. The focus of these doctors is often on prevention and longevity, trying to keep the patients healthy and functional for as long as possible instead of being financially incentivized by sickness.
Many of these doctors use hormones extensively and have been doing so for decades in thousands of patients. They often balance multiple hormones simultaneously using small physiological dosages. There certainly are risks (as there are with any other therapy) but if doses are physiological, hormones properly balanced with each other, and the proper delivery route used, the risk is much smaller than what conventional medical “wisdom” leads people (and doctors) to believe.
For a long time, many of these doctors have practiced in the background, largely outside the established medical system, and predominantly served the rich and powerful, though it seems that times are changing.
Hopefully, proper hormone replacement will be more widely accessible in the future beyond the domains of “alternative”, “functional”, “complementary”, or anti-aging medicine.
Unfortunately, many people do not like hormones because they prefer “natural” treatment instead. They would rather ingest truckloads of unnatural herbal supplements than administer the natural hormones our physiologies evolved with for millions of years.
Personal experiences
Over the years, I have experimented with a large number of hormones. Feel free to click on the links below to read about my experience in more depth.
The difference between “transformative” and “supplementary” hormones do not relate to the general importance of a particular hormone but rather to how much a hormone has changed my life at the point in time I experimented with it. All the “transformative” hormones have been life-changing in one way or the other and I would not be today where I am now without them. Conversely, all the “minor “supplementary” hormones were interesting but not life-changing in any way.
Transformative hormones
Supplementary hormones
- My Experience With “Non-Standard” Hormones (GH, Insulin, EPO, Estradiol, Oxandrolone, Oxytocin, etc.)
- Growth hormone
- Insulin
- EPO
- Estradiol
- Oxandrolone
- Oxytocin
- ADH
- Pregnenolone
- DHEA
- Teriparatide
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Strategies I follow to optimize my hormones naturally
- I optimize my sleep.
- I make sure I eat enough calories (for me, about 3500-4000kcal per day), with enough good carbs and good fats. Whenever my caloric intake is insufficient, some of my hormones decline, including sex hormones, thyroid hormones, and IGF-1.
- I stopped any kind of fasting (both multi-day fasting as well as intermittent fasting) in part because fasting can cause all sorts of hormonal issues.
- I put a prime on exercise – but I make sure not to overdo it.
- I used to make sure that I do not dip below 14% body fat. Whenever I did, a number of hormones took a hit. Starting semaglutide allowed me to tolerate about 2% lower levels of body fat without hormonal deterioration. I now circumvent this problem altogether by taking a low dose of metreleptin sufficient to mimic a body fat percentage of about 15-20% (but without the aesthetic and metabolic downsides). The last time I checked, my body fat percentage was 10.6% (DEXA).
- I take a couple of supplements to prevent nutrient deficiencies (discussed here).
- I run an extensive hormone panel once per quarter (discuss here).
I discuss hormones & aging in more detail here.
Hormone deficiencies often go unrecognized
A non-minor number of individuals are hormone deficient. A large number of external or internal conditions can cause endocrine imbalances. These include insufficient food intake, lack of sleep, excessive exercise, fasting, ketogenic diets, low body fat percentage, immune system issues, nutritional deficiencies, high stress levels, or “healthy things done in excess”.
Quite often, people go doctor-shopping but they often cannot find anything. There are two primary reasons for this:
- The specializations and subspecializations in medicine have produced many doctors who are blind to everything out of their narrow domain and therefore hormones are rarely properly checked.
- Lab values often come back “normal” and therefore many hormone-deficient patients fly under the radar of the current medical system of doctors who just look at values that are flagged.
How to check for hormone deficiencies?
All of the major hormone deficiencies (thyroid, sex hormones, cortisol, leptin, growth hormone) have partially overlapping signs and symptoms. These include fatigue, low mood, low libido, bad sleep, brain fog, low motivation, and weight gain, and sometimes even anxiety or depression. However, these signs and symptoms are shared with many other non-hormonal conditions as well.
Because symptoms are often unspecific, getting a decent hormonal panel is a reasonable starting point.
Here is what I would test for:
- TSH, fT3, fT4 (optional: reverse T3)
- Total testosterone, SHBG, estradiol (free testosterone can be calculated from total T & SHBG & albumin)
- DHEA-S (a marker for adrenal status)
- IGF-1 (a marker for nutritional status & growth hormone secretion)
- Leptin
- Vitamin D (yes, vitamin D is a hormone as well)
Then, in combination with test results, going through the signs & symptoms of a specific hormone deficiency. Some of these signs & symptoms were listed above.
A note on blood tests
Blood tests measure what is in the blood. They do not measure cellular action, which is what it is all about. Therefore, when it comes to endocrinology, blood values matter just as much as physical signs (e.g., body hair, heart rate) and symptoms (e.g., fatigue, low libido). This was something that was hard for me to wrap my head around.

Firstly, blood tests only measure hormone concentrations at a specific snapshot in time. For example, simple things such as eating much less for a couple of days will alter hormone levels.
Secondly, blood tests do not necessarily map 1:1 to hormone action because hormone sensitivities differ between people. For example, my testosterone of 600ng/dl is not equal to your testosterone of 600ng/dl (regardless of free levels). Me and you could have different polymorphisms of the androgen receptor (AR). Or we could have different AR densities. Or we could have different versions or amounts of 5-alpha reductase (an enzyme that converts testosterone into the more potent DHT). Or we could have different versions of 3-alpha-hydroxysteroid dehydrogenase (an enzyme that converts androgens into less active metabolites). Or we could have different quantities of androgen-induced changes in transcription factors. Or we could have different accessibility to androgen-sensitive genes. And the list goes on.
All of us have differences in binding proteins, metabolism, cellular sensitivity, function and quantity of receptors, nuclear cofactors, gene methylation patterns, etc. Because of these interindividual differences, optimal hormone levels often differ between individuals – and so do the effects an individual experiences upon the exogenous introduction of a hormone.
All of this makes it seem like blood tests are useless. They are not. Blood tests are highly valuable. However, one needs to keep in mind that, like any other diagnostic test, there are caveats.
It is a mystery why not much research has focused on hormone biomarkers, of which the most promising candidates are probably hormone-specific changes in certain target genes.
A note on reference ranges
Most doctors are trained to recognize only the extremes of hormone production – either “very low” or “very high”. Medical reference ranges are purely statistical ranges. By definition, 2.5% of people are below and 2.5% above are above the range.
This is an issue because a lot of people who could potentially benefit from hormone replacement therapy fall into the somewhat arbitrary “perfectly normal” range, which is not necessarily the “optimal” range.
In my experience, when doctors look at my blood work, they usually treat it as an “all-or-nothing” issue. If I fall anywhere within the “normal” range, a doctor will tell me everything is great. However, if I am just slightly above or below an arbitrary number, they will tell me something is wrong.
I guess that many people who seek out doctors for problems with hormone deficiencies at their root cause do not fall below the medical reference range and thus often fly under the radar of the current medical system that just looks at values that are flagged. Their values come back “normal”. However, normal for someone 30 years their senior.
For example, the reference range of free thyroid hormones spans a range of factor three. Someone with three times as much thyroid hormone in their body will quite likely feel and function differently compared to someone with only one-third as much – despite both being considered “normal” by the conventional sick-care system.
Hormone crosstalk
The endocrine system is an intricate system. Turn one gear and many others are set in motion as well.
When one of the major hormones is modified, there are many multi-layered second and third-order effects on many other hormones. Interactions occur on many levels, including the hypothalamus & pituitary gland, other endocrine glands, the level of hepatic binding proteins, and ultimately the level of gene expression.
For example:
Thyroid hormones, IGF-1, and growth hormone are all known to stimulate other hormone axes – both at the level of the hypothalamus and pituitary gland as well as at the level of the endocrine gland. Furthermore, thyroid hormones and IGF-1 stimulate cellular activity and therefore they tend to increase the “sensitivity” of target cells to the effects of other hormones. Thyroid hormones stimulate the synthesis of binding proteins (e.g., SHBG) whereas growth hormone and IGF-1 decrease them, which may result in small changes in free hormone levels. Thyroid hormones affect aromatase activity and therefore modulate estradiol levels. Growth hormone stimulates IGF-1 synthesis, which then stimulates an enzyme called deiodinase II (which increases conversion of T4 to T3), and an enzyme called hydroxysteroid dehydrogenase type II, which inactivates cortisol to cortisone.
Analogous interactions are known for other major hormones.
These effects are just the tip of the iceberg as each of the major hormones affects hundreds of genes, and many of the molecular effects have only been roughly elucidated.
Do hormones produce “tolerance”?
The introduction of exogenous hormones is always accompanied by (some) endogenous suppression, which, however, is not the same as tolerance.
Many hormones act on gene expression, either because they act on nuclear receptors (e.g., sex steroids, thyroid hormones) or powerful cytokine receptors directly linked to transcription factors (e.g., leptin, EPO, growth hormone).
Compared to stuff that acts on G-protein-coupled receptors (the targets of most neuropharmaceuticals or recreational drugs), there is much less tolerance to these direct changes in gene expression, which is the most downstream level possible.
However, there will be some tolerance to some effects on neurotransmitter systems (which is what many people are after). For example, after starting testosterone, many experience energy, motivation, and even slight euphoria. These effects are mostly due to testosterone affecting neurotransmitter systems, particularly the dopaminergic system.
Unfortunately, changes in neurotransmitter systems and the ensuing “honeymoon period” are somewhat short-lived. After raising the dose, individuals will often “feel” much better for a short period of time (usually on the order of weeks). However, after a couple of weeks, the brain-based hedonic treadmill takes over and neurotransmitter signaling drifts back toward baseline.
Unfortunately, “how we feel” is not the best guiding factor to determine hormone dosages. “How we feel” depends entirely on the nervous system and we do not “feel” whether the liver, heart, kidney, immune system, etc. are in a hypo- or hyperhormonal state. Therefore, hormones should not be dosed solely depending on “how one feels”.
Hormone tunnel vision
If hormone levels are low, then replacing the hormone in question in a balanced way is a safe, causal, and effective way to rectify the symptoms associated with hormone deficiency. However, it seems that many people are chasing symptoms (e.g., libido, energy levels) and end up replacing hormones in supra-physiological doses even though the putative hormone deficiency was not the root cause of their symptoms in the first place.
For example, guy X might be somewhere around the 40th-50th percentile of testosterone levels. He believes he has every low-T symptom under the sun including fatigue, difficulty losing weight, poor self-confidence, low libido, etc. He is dead certain that his low testosterone levels are at fault for his symptoms and self-diagnoses with “low T”.
Guy X starts to replace his testosterone. Dopamine levels rise and he feels great for a couple of weeks. He believes that he has found the root cause. But as his dopaminergic system adapts, he is soon back to square one. Now the raise, raise, raise period begins, during which he always feels good for some time after every raise, assuming he has simply not raised his dosage enough, even though his levels of testosterone are far above the normal range already.
Gradually he starts to feel “like shit” again. Now he starts to blame the rising estrogen levels. He titrates back and forth testosterone and aromatase inhibitors, assuming he simply has not found the holy balance yet.
However, testosterone was never his issue to begin with and the initial ‘Low T’ problems come back after the honeymoon period. The issues are often complex processes in the nervous system, which might be unrelated to hormone levels. Quite often, the root cause is undiagnosed low-level dysthymia or depression (which is not the same as “suffering”).
If one’s issue is primarily of neurotransmitter or central origin, replacing hormones can definitely bring about (temporary) improvement, particularly replacing hormones in supraphysiological doses in order for them to have supraphysiological effects on various neurotransmitter systems.
Nonetheless, in these cases, hormone replacement is not addressing the root cause and improvement will be incomplete and temporary, even though people can often feel much better over a short period of time.
Abusing hormones for symptom relief is not just unhealthy, but can be quite dangerous and cause irreversible changes in a number of organ systems. Furthermore, it is trading in short-term vitality for long-term health.
Unfortunately, the symptoms of hormone deficiencies overlap with the symptoms of low-level depression and other conditions that are only weakly related to the endocrine system.
In fact, many people with symptoms of hormone deficiencies (e.g., fatigue, low energy, bad sleep, anhedonia,) do have low-normal hormone levels. Some people choose to replace hormones, only to find that it does not bring lasting relief. The meteoric rise in TRT is just one example.
In my opinion, many people would be much better off in terms of safety, health, efficacy, and reversibility if they made major changes to their lifestyle or interfered with neurotransmission directly. For example, I know of two people who switched from testosterone replacement therapy to bupropion, with better and more sustained effects on energy, mood, motivation, and sex drive – the reason why they sought testosterone replacement therapy in the first place. Furthermore, bupropion is leaving most organ systems untouched that would be adversely affected by testosterone.
In sum, some people fare better with antidepressants. As always, the drug regimen of choice is best found through cautious empirical self-investigation.
Hormones can be replaced for life without adverse effects, if they are replaced well.
Recently, I saw a patient who was 81 years old and she was taking 150mcg of thyroxine (T4). She had been on this dose for over 30 years because of total thyroidectomy. Her TSH is completely suppressed and had been this way for decades. She felt “phenomenal” (actual quote), was quite lively, did not need blood pressure or lipid-lowering medication (perhaps due to her higher levels of thyroid hormones) and was definitely healthier than most other 80-year-old patients.
Similarly, I recently had a patient who had a six-pack at 75 years of age. He was type I diabetic and had been replacing his insulin since he was 14, meaning that for 60 years he had been relying entirely on exogenous hormone replacement to survive. Other than the insulin and pantoprazole, he did not use any other medication. He was quite vital, had a full head of hair, and exercises every day. Compared to most other Type I diabetics, he uses only very low doses of a basal insulin (20IU per day) and primarily uses walking and exercise as his primary method of controlling postprandial glucose excursions.
The point I am making is not that these people may have gained an advantage because of their exogenous hormone replacement (which may or may not be true) but rather that, given that hormones are replaced well, one can replace them for life without obvious adverse effects – such as these two individuals, who were relying to 100% on exogenous thyroid hormones and insulin respectively for multiple decades.
Many people I meet are of the opinion, that exogenous hormone replacement must be bad because it is “artificial” and “natural” is better. However, our human bias for preferring “natural” leads us astray, at least in this instance.
Why I do not use peptides
I discuss my personal experience with peptides and why I am literally scared of using them in more detail here.
Hormones & longevity
Hormones and their effects on longevity are discussed here.
How I Biohack My Vitality
This article is a subsection of How I Biohack My Vitality.
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.