

Sometimes I wake up and I am immediately ready to go. My energy is high, my mood is good. I feel strong and motivated. On these days working is fun. After a day of work, I go to the gym, work on projects, and do something social in the evening.
Other times I wake up and I feel like crap. Either because I have slept particularly badly (most common reason) or something is off with my neurobiochemistry or hormones. Anyway, on these days, everything is a drag. I look forward to finishing work. If I am not working, I procrastinate and get lost in the news or other things that do not particularly interest me. I drag myself to the gym, and I need to take yohimbine (my caffeine replacement) to have enough energy to enjoy the social stuff.
Fortunately, I never have “What is the point?” days but I can see that if low-vitality days become low-vitality months or even low-vitality years, such a mindset might take hold eventually. Anyway, no matter the cause, I feel that I am twice as productive and my moment-to-moment life is twice as enjoyable when my vitality is good.
It is my deep-seated belief that if I improve my vitality, particularly energy levels, a lot of other things in my life will improve automatically because every waking second I think, feel, and act differently.
The best part is that other than designing protocols for vitality improvement, I do not need to know anything. Given that the protocols in place are correct, the benefits in my life are automatic. This is similar to meditation. Just do the activity correctly, and you will profit automatically in daily life even if you did not know any theory behind it.
The key to changing my life is changing my habits. Big achievements are about the tiny, non-sexy things that I do every day. James Clear preaches this in the book “Atomic Habits” and I do not disagree. But guess what: If I feel awful all of the time, changing my habits, let alone sticking to them, is quite tough.
My habits at any given moment are partly a function of my energy and mood, and, in my opinion, having good energy and mood is a prerequisite to living a fulfilling, healthy, and productive life in the first place.
Relatedly, improving my vitality is the single biggest step I can take towards improving my life as it has a huge impact on virtually every other area, including my relationships, dating, work, drive, happiness, etc.
The Oxford Dictionary defines “vitality” as “the state of being strong and active”. For the sake of this article, I will define vitality as a catch-all-term encompassing four things, which are all intricately related:
- Health
- Energy levels
- Mood
- Motivation
Essentially, it means having the neurobiochemical set-up of a kid.
If I am tired or unmotivated, living a healthy lifestyle, getting things done, or enjoying my life is not in the cards. Conversely, if I am healthy, energetic, and in a good mood, I am happier, more productive, more self-disciplined, and, I believe, also a better human being. This biology-mediated automatic change in my emotions, thoughts, and behaviors is quite unlike any intentional self-improvement stuff.
This article is a collection of numerous non-lame biohacks. Some of these have changed my life and the life of many of my friends. I will not bother with “8 obscure herbal supplements you need to take” or “17 superfoods you need to eat”. I will only cover stuff that works.
Disclaimer
The content available on this website is based on the author’s individual research, opinions, and personal experiences. It is intended solely for informational and entertainment purposes and does not constitute medical advice. The author does not endorse the use of supplements, pharmaceutical drugs, or hormones without the direct oversight of a qualified physician. People should never disregard professional medical advice or delay in seeking it because of something they have read on the internet.
Background
Over the course of my life, I was held back by my biology many times. At various points, I struggled with low energy levels, bad mood, lack of motivation, trouble concentrating, brain fog, terrible sleep, or a ravenous appetite. More often than not, these were problems of the body and not the “mind”.
For the past decade or so, it has been my hobby to hack my biology. If I want to improve something, I research it, decide on an intervention, implement it, track the results, and draw conclusions to find out whether something works for me or not.
More than once I realized that many of the best changes I can make are unknown until I make them. In this regard, feeling “fine” is potentially a dangerous attitude because it prevents me from getting to know how much better I could feel or function.
In his book Antifragile, Nassim Taleb is a big proponent of trial and error, which he calls “tinkering”, as a way to figure things out and expose yourself to large potential upsides. Similarly, my best “innovations” came from making an educated guess and simply trying things out. While about 95% of my experiments were failures, the remaining 5% easily made up for them, and I am deriving benefits to this day.
Biological intervention is always a complex calculation of tradeoffs and carries significant risks, although there are significant risks from doing nothing as well – this point is often neglected. For me, the potential gain from (prudent) self-experimentation has thus far vastly outweighed the risks and side effects associated with it.
If I find something that suits my individual biology, needs, and preferences, I can potentially derive compound interest in many domains of my life for many years to come. Furthermore, the non-zero-sum nature of my world implies that if I improve my health, happiness, performance, and productivity, it benefits not just me, but also those around me – a concept known as “moral bioenhancement”.
I would go as far as to argue that if I were low energy and depressed all of the time, it would be quite unethical not to intervene, because the state I am in has direct and indirect effects on my fellow humans, and not taking action is a form of action in itself.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Outline
This article is long. I have divided it into multiple parts.
Part I: My Protocol & Ranking – What I currently do & take and a ranking of the interventions discussed later in the text. This also serves as a high-level overview of what follows.
Part II: Lifestyle – I discuss the basics in more detail.
Part III: Nutrients, supplements, blood testing – I discuss the supplements I take and my approach to blood testing.
Part IV: Hormones – I discuss the unparalleled power of hormones, and my personal experience with them.
Part V: Antidepressants (and related molecules) – A bunch of molecules that are potentially useful for enhancing certain aspects of well-being.
- Detailed discussions of individual molecules
- Can stimulants and antidepressants be taken forever?
- Thoughts on modern psychiatry
- Case reports: Examples of cases that are hard to treat
Part VI: Stimulants – These can be useful to take occasionally.
- The dark side of stimulants
- Principles for safe and sustainable use
- Detailed discussions of individual molecules
- Noteworthy molecules stuck in pharmaceutical pipelines
Conclusion: On Butterflies, Upwards Spirals, And The Most Powerful Force In The Universe
A short summary of the article can be found here.
Guiding principles
Before delving into practical aspects, I will now discuss four guiding principles that provide the rationale (the “why”) for the remainder of this article.
Principle #1: Biological factors are important.
A good friend of mine is doing quite well for himself. He is in his final year of med school, has already started two businesses, is great at sports, and an active dating life. He attributes much of his (conventional) success to his hard work and “mindset”. He does not understand people who are lazy and who do not try hard at the only life they can be sure of having.
Then, long-COVID hit and his 90th-percentile energy levels, mood, and drive were instantly taken away from him. Suddenly, maintaining a great “mindset” and hard work was much harder. He was forced to realize how easy life had been for him, in part because he had always been feeling very energetic, enthusiastic, and motivated, all of which he had taken for granted.
Not until he had lost what he did not even know he had, did he realize how lucky he had been in the biology department. Now, for him, life is hard and sucks and he is only slowly getting better. Perhaps subtly looking down on “lazy” people was not fair after all because there were underlying conditions that had enabled him to be good at life. For reading about how the story continued and how he is doing now, click here.
Similarly, let’s imagine I had my best, most vital hour of the day (for me, usually the first hour after waking up) extended to the entire day. 7 days a week. 365 days a year. Where would I be 10 years from now (psychologically, physically, financially, socially, intellectually)?

Biological factors ripple through my life in the same way an earthquake ripples through the Earth’s crust. My energy levels, mood, health, motivation, concentration, emotionality, memory, and cognition (all of which have strong biological underpinnings) affect me every waking second of every single day.
These biological factors then influence my thinking patterns, the lifestyle I lead, the decisions I make, the relationships I have, my productivity, my happiness, and much more. Whatever I want in life, whether that is creating, contributing, achieving a specific goal, or simply living life to the fullest – my biological makeup can make or break it.
Furthermore, everything I do has ripple effects that spread far beyond where I can ever see them. Something I do may affect the way someone else interacts with others, which in turn may affect how they interact with others, and so on and so forth.

I change the path of all of the lives I touch, sometimes imperceptibly, sometimes drastically, even though in most cases I will never realize it. Again here, biological factors will co-determine my impact on the world and others.
I discuss this principle in the form of a story in more detail here.
Principle #2: My mental and physical operating system is outdated.
When I was a child, I imagined archetypal nature to be this caring, nursing mother. However, as I learned more about the world, it turned out that romantic Mother Nature is rather cruel and callous. The Earth’s biosphere in its original state is incapable of supporting human flourishing as it is naturally infested with predators, parasites, food scarcity, and a variety of diseases.
Given that this was the evolutionary backdrop against which my ancestors’ bodies and minds developed, I now find myself in an utterly unnatural environment. In the same way that humans invented technologies to tailor the biosphere to human flourishing, I can use technologies (e.g., pharmacology) to update my body and mind to the contingencies of the modern world.
When an animal is living in the environment & conditions in which it evolved, the gratification of its drives & instincts usually maximizes reproductive fitness. However, the instincts of my Stone Age mind are not a reliable guide in the modern world for what is “good” for me.
The life that I experience today is not the life that my primate DNA had been prepared for. My body and mind have evolved for a very different era and have not yet adapted to the modern environment, which includes artificial lighting, pollution, processed food, appetite being set to excessive levels, a sedentary lifestyle, living beyond the age of 50, prolonged stress, intense schedules, loneliness, social media, a requirement for constant mental alertness, an altered circadian rhythm, among others.
Because my body and brain evolved for a different environment, my biochemical machinery and physiology are outdated and not well suited to the unnatural modern ecosystem I currently live in. However, for the first time in history, technology allows me to overcome some of these biological limitations.
For example, in the past, food was usually quite scarce and therefore, my ancestors evolved to be drawn to junk food, overeating, and storing fat. However, this is maladaptive in the modern-day environment. The fact that modern food has been engineered to trigger overconsumption surely does not help either (sweetness; umami; mouthfeel; caloric density; flavorings; crunchiness; etc.).
My primitive brain is therefore mismatched to this modern ecosystem of convenience and abundance and an orchestra of mechanisms wants me to pig out. For many members of my species, food addiction, obesity, type II diabetes, and cardiovascular disease are a consequence.
As soon as I started to use GLP-1-agonists to update my homeostatic and hedonic aspects of food intake, cravings and food-related thoughts were gone. Instantly.
This also makes me wonder whether we humans are generally unfit for the future in the same way our “thrifty genes” are unfit for the present. Fortunately, the ability to discover and use explanatory knowledge (a.k.a. science) gives us humans the power to transform nature and ourselves – limited only by the laws of the universe.
In this manner, I can use “biohacking” to update my biological operating system to the contingencies of the modern world. In my view, using technology to counter these limitations is just as natural as living in the current unnatural world in the first place. If some upgrading happens along the way, I do not mind.

Principle #3: Technology is the driver of human progress.
For the past 50 years, pharmacological and technological self-modification allowed athletes to vastly surpass human peak performance in pretty much every sport. Similarly, it is thought that drive and mental performance went up on a population-wide level after the introduction of caffeine around the time of the industrial revolution.
We as a species made it this far because we continually shared information, collaborated, and engineered solutions to problems and conditions we wanted to change. Without this ability, my ancestors would presumably not have progressed beyond living in trees, let alone caves. In fact, throughout history, most humans have lived in a sick society: malnourished, infected, and often mentally impaired. Enter science and technology.
For a long time, humanity had been using science to study how the world works, and then applied the discoveries of science to achieve specific goals. The ability to discover and use explanatory knowledge gives humans the power to transform nature and themselves – limited only by the laws of the universe.

Scientific materialism is our best story of the world. Hence, technologies work. In terms of medicine, pharmaceutical drugs are among humanity’s major technologies. By using knowledge of how the body works, humans create molecules that perturb the body’s molecular signaling to produce a desired effect.
Like any other technology, pharmaceutical drugs have both risks and benefits. However, as with other technologies, the upsides can outweigh the downsides if the technologies are applied wisely.
For more: Paradise Engineering: The AGI Aspect I am Most Excited About
Principle #4. There are better and worse drugs.
A friend of mine was heavily addicted to weed, which more or less derailed his life. He had a hard time coming off and I suggested the temporary use of bupropion to help him quit. In part thanks to the boost in energy, mood, and motivation, was he able to come off quite quickly.
Evolution’s goal was to increase reproductive success – and not personal well-being. Natural selection does not care about how genes are passed on, only that they will.
As a result, humans tend to be naturally in a state of constant low-level dissatisfaction, because being low-level dissatisfied was probably more adaptive than being content or blissed out. In part because evolution did not prioritize emotional well-being, humans have turned to drugs ever since.

Large parts of the population currently consume either alcohol, cigarettes, or toxic amounts of sugar – or a combination of these. Millions of others consume weed, amphetamines, opioids, or cocaine. These drugs provide temporary pleasure but almost always have negative long-term consequences when used continuously.
Viewed in terms of mortality, morbidity, or life enjoyment, I am likely better off if I switched to “good drugs” instead, namely drugs that have long-term beneficial effects on myself and my loved ones (“moral bioenhancement”). From personal experience, I can say that these drugs do exist.
Furthermore, using the fruits of modern medicine wisely can help me establish a happier baseline state, and create a life that is fulfilling in itself, which makes using pleasure shortcuts less tempting in the first place.
Part I. My Vitality Protocol and Ranking
I believe that I have only one chance to live, and I want to do it in the most fulfilled and meaningful way possible. Considering that the human mind creates every part of my reality (in fact, is identical to my reality), working on what is going on in there is a top priority.
Because I want some control over my emotional and cognitive state—beyond what mindfulness, reframing, and psychotherapy can offer—I also leverage my biology directly, including making strategic lifestyle choices, hormone optimization, and utilizing pharmacology. While some may think of this as “cheating”, given that the outcomes of my mind are all that I have to offer to others, I believe this is an ethical thing to do.
In this section, I lay out my current protocol, which remained more or less unchanged for quite some time now. At the end, I try to rank the interventions discussed.
Table of contents
My current protocol
For a long time, I have put a prime on personal growth. I have listened to tons of podcasts, read lots of books, and have gone to psychotherapy. However, the things that really helped me were rarely pieces of “knowledge”. Once everyday life hit, most of what I had “learned” was swiftly forgotten.
For me, more “knowledge” was not the answer. Knowledge mostly helped if I could practically apply it. For example, knowledge about how to remove distractions, how to redesign my environment, why I should quit social media, and why I should complete my most important task of the day first.
However, what really stood out was knowledge of my biology and how to optimize it. Because biological intervention changed my thinking, behavior, and life quite unlike anything else.
My primary motivators for starting biohacking were (presumably) curiosity, wanting “more” out of life, and a feeling of not being good enough. In retrospect, had I consistently “felt fine”, it would have prevented me from self-experimentation, possibly ending up being a net detriment.
Even though self-experimentation is risky, some of my biggest mistakes and failures resulted in the most important “innovations”. In this way, failures and mistakes were an important stepping stone towards finding something that suits my individual preferences and biology.
In the past, I have relied more on stimulants than I should have. Now, I am much more interested in interventions that improve my baseline vitality (the way I feel and function on a daily basis) and I am turned off by interventions that worsen it. In my experience, when it comes to short-acting drugs, there is rarely a biological free lunch (e.g., drinking coffee today has me paying for it tomorrow).
Also, I gave up on the idea of finding a perfect final state. For such a state to exist, I would need to be in an unchanging environment, which is neither possible nor desirable. Therefore, I adjust as needed depending on my physiology, preferences, priorities, and life circumstances.

Nonetheless, similar to how many investors switch from day trading to more long-term investments, over time I switched from fiddling with my interventions a lot to a more stable protocol, which I now vary rarely.
I always assumed what works for me must work for anybody else. However, I came to realize that this is not true at all, and people respond very differently to the same things – sometimes radically so.
I found that my response to a certain intervention is a very individual thing, and it is awfully hard to tell in advance whether I respond well to something or not, regardless of what doctors, the medical literature, or anecdotal online reports make me believe. The only sure way to figure out how I respond to something is to try it.
For me, all of the following interventions have stood the test of time, meaning that I have been doing them consistently for at least two years (most of them for longer) and still derive benefits. This is quite unlike most of the online reviews I usually encounter, where someone tries out X for one week, hops online and writes a glaring review claiming “X changed my life”, and then vanishes from the face of Earth.
So, without further ado and in no particular order:
Sleep
Out of diet, exercise, and sleep, sleep is the one I am most sensitive to. When I am sleep-deprived, I am a worse version of myself in almost every way, and my area-under-curve levels of productivity and well-being are significantly reduced. Basically, if my sleep is awful, so is my entire day.
I sleep in a cold, dark, and quiet environment. I also use earplugs and a cooling blanket. Before sleep, I take magnesium and glycine. I usually sleep from 10.00 to 6.00, and my sleep quality is quite sensitive to going to bed later than usual.

Most nights, my sleep is quite good, and I wake up refreshed without an alarm. Upon waking, I use a 10.000 lux daylight lamp while doing my morning routine.
I discuss my sleep optimization routine in more detail here.
Exercise
I put a prime on exercise. Exercise improves my sleep, energy levels, mood, metabolic health, and cognition. Whenever I do not exercise for a day, something is missing. And if I do not exercise for multiple days in a row, I get antsy, irritable, and my energy and mood drop significantly.
I try to integrate different kinds of exercise (resistance training; aerobic; anaerobic; mobility) as they all have partially independent benefits. The best all-in-one solution I have found so far is CrossFit, which I thoroughly enjoyed.
Thanks to CrossFit I have also undergone “fitness menopause”, changing my focus from aesthetics to vitality. After 18 months of doing it regularly, I decided to stop and switch to more longevity-focused exercise considering that many people seem to eventually get hurt with CrossFit.
I now alternate between steady-state cardio (zone II exercise) and the gym. Recently I have also implemented a mobility routine focused on lower body mobility.
I discuss my exercise regimen in more detail here.
Diet
I have experimented with many different diets. Nothing stuck. Sometimes I felt great initially, but over time I felt worse, for example with intermittent fasting or a ketogenic diet. For me, how I feel is more important compared to how well a diet performs “on paper”.
Furthermore, for me, going on semaglutide (explained next), made dietary experimentation obsolete, and I now only try to adhere to three loosely held rules.
- I cut out most of the processed food and sugar (80/20 principle).
- I adjust my carbohydrate intake to my leanness and activity levels.
- I make sure to eat a sufficient number of calories.
I believe that, for me, these rules are sufficient to get about 80% or so of the benefits that are maximally attainable through dietary intervention. I believe that if I am already on a reasonable diet, dietary intervention is a low-leverage lever to pull, especially compared to sleep and exercise.
I particularly like Huel shakes with lots of olive oil, which give me stable energy and are convenient to prepare. With semaglutide & Huel, I outsourced 80% of my nutrition.
I discuss my diet in more detail here.
My TRT Lite Protocol
I have been on my TRT lite protocol now for a little over a year. I can safely say that increasing my levels of testosterone & estradiol has increased my quality of life and probably also my health. While it is not “life-changing” by any means, overall I feel it to be quite a strong net benefit to multiple aspects of my life.
Benefits I have noticed include more energy, slightly less need for sleep, greater emotional intensity, an easier ability to build muscle, and a higher libido.
My protocol does not include testosterone itself but a low dose of hCG combined with a low dose of finasteride, which I feel gives me the best of both worlds. I discuss my experience and my protocol in more depth here: My TRT Lite Protocol
I take a low dose of finasteride despite having no signs of hair loss whatsoever: Experience & reasoning here: My Experience With Low-Dose Finasteride to Lock In My Prime
Supplements
I use quite a few supplements. Other than vitamin D, fish oil, and magnesium I am not sure whether they are of any benefit, and I mostly take them with a just-in-case mentality.
Honestly, I kind of feel bad about taking them because I have so little data. However, I feel equally bad about not taking them because they all have theoretical benefits in a variety of domains. For now, I simply close my eyes and hope that they do more good than harm.
I discuss the supplements I take, and why I take them, in more detail here.
Blood tests & monitoring
Every quarter, I get extensive blood work done and monitor a number of things, ready to intervene accordingly. I do a full-body MRI every three years and a DEXA scan once to twice per year. I track my sleep and exercise parameters and occasionally also my blood glucose with the use of a continuous glucose monitor (CGM). I also have ready access to great doctors from multiple fields and some of them are among my best friends.
I discuss the blood tests I do in more detail here.
Longevity interventions
My goal is to live a long and happy life. If I had to choose between longevity and vitality, I would choose vitality without a second thought. Fortunately, these two are not necessarily mutually exclusive.
I describe my approach to longevity in detail here.
Thyroid hormones
Until very recently, I have been supplementing with low doses of thyroid hormones for about six years despite not having hypothyroidism.
Thyroid hormones increased my baseline vitality by a good amount, particularly the addition of a small amount of T3 (the active thyroid hormone that is rarely prescribed). I particularly liked their effect on morning energy levels. Overall, for me, thyroid hormones made life a little bit easier and better.
I recently stopped taking them because I found that the drastic increase in caloric intake for a year or so had boosted my thyroid hormones from the low-normal to the high-normal range, and I felt that the additional T3 dehydrated me and made me a tad more restless. Time will tell whether I go back to thyroid hormones or not.
I discuss my experience with thyroid hormones in more detail here.
Moclobemide
Despite not having depression or anxiety, I have experimented with many antidepressants and similar molecules aiming to enhance my productivity and well-being (“cosmetic neuropharmacology”) in the same way many others use e.g., caffeine for similar purposes.
I found low doses of bupropion and vortioxetine useful but the one I liked the most was a low dose of moclobemide. It felt natural and it did not mess with my appetite, libido, or sleep.
On moclobemide, I had more energy, I was almost always in a great mood, and anxiety and worrying were mostly absent. However, I was also less “deep”, a little less capable of feeling profound feelings, and slightly less sharp. At the very least, it is fair to say that making me “happier” than I would normally be is a double-edged sword. Eventually, because of the slight emotional and cognitive blunting, I decided to come off, though one day I might return to it.
After some time off moclobemide, I realized that my life is better on it. Moclobemide makes me a slightly happier, a slightly more productive, and slightly “better” human being. I take a very low dose of rasagiline with it to balance out the dopamine-serotonin ratio. I take both MAO inhibitors at very low, subclinical doses. I take 2×37.5mg of moclobemide per day and 0.025mg of rasagiline per day.
I discuss my experience with moclobemide in more detail here.
Semaglutide
I naturally have quite a strong appetite, and throughout my life, I have wasted a lot of energy and brainpower on food. The addition of a low dose of semaglutide, which modifies the homeostatic and hedonic aspects of feeding, has been a huge hack for my productivity, looks, and well-being.
The major downside is that semaglutide makes it hard to meet my caloric requirements if I do not count calories. I do not use semaglutide to lose weight (in fact, I actively try not to lose weight) but rather to decouple appetite from caloric intake. Thus, semaglutide helps me to be in charge of my drives and not the other way around, which I think is a very human thing to do.
Other than its cost, the need to count calories, and some loss of pleasure from eating, for me, there were no side effects as of yet (at least for the two years I have been using it). My resting heart rate is unchanged and I even built about 3-4 kg of lean muscle on it. I currently only use a very low dose (2 clicks per day, which is about 0.2mg per week – so a single pen lasts me about half a year).
After about 3 years on it, I am currently off semaglutide because I want to gain weight.
I discuss my experience with semaglutide in more detail here.
Hypnotics
Occasionally, I use a low dose of a sleeping pill. I feel that if used sparingly, the risks and side effects of poor sleep are greater than the risks and side effects associated with hypnotics. I have experimented with many hypnotics, though few have stood the test of time. Currently, I use two hypnotics occasionally:
- On days when I want to ensure a great sleep, such as before an important meeting, I take 1mg of eszopiclone. For me, this medication virtually guarantees a restful night’s sleep with no hangover. I do this about once per month.
- On days I have a particularly tough time falling asleep, I use ¼ of a 0.25mg triazolam pill sublingually, which has me fall asleep within a couple of minutes. I do this about once per week.
However, long-term use of CNS depressants, such as benzodiazepines, Z-drugs, gabapentinoids, and antihistamines, is associated with progressive cognitive impairment, which does not seem to be explained by residual confounding.

I discuss sleeping pills in more detail here.
Caffeine
I mostly avoid caffeine because it not only interferes with my sleep quality but also makes me less alert whenever I do not have it. When I consume caffeine, which is perhaps once per month, I preferably consume it in the form of white tea or diet coke, which has comparatively little caffeine and does not stain teeth.
I discuss my experience with caffeine in more detail here.
Modafinil
In the past, I often used modafinil to help with studying and being more productive, but now I very rarely use it because it hampers my creativity, and on it, I tend to do things more thoroughly than intended, which usually ends up being time-robbing instead of time-saving.

Now I only use it perhaps once or twice a month, on days I slept particularly badly or little. Like other stimulants, frequent use worsens my baseline. I feel that stimulants in general are mostly “borrowed” energy, and modafinil is no exception.
I discuss modafinil in more detail here.
Nicotine
On work-heavy days I usually consume about 4-6 cigarettes’ worth of nicotine in the form of nicotine replacement products. Nicotine helps me with alertness, cognition, memory, and makes boring tasks more fun. The major downside is that nicotine is addictive, though the addictiveness depends in part on the delivery vehicle.
Warning: Nicotine is addictive and setting oneself up for a potentially life-long addiction is not to be taken lightly, even if the health effects of nicotine itself are far below those of smoking cigarettes (which is a low bar to meet).
I make sure that my nicotine tablets or gums are flavorless. For me, having something sweet or flavorful in my mouth measurably decreases my cognition (for evolutionarily obvious reasons as an ongoing pleasure reaction decreases cognition so that the animal keeps doing whatever adaptive thing it is currently doing).
I discuss nicotine in more detail here.
Non-biological self-improvement
I prioritize my community, do meditation, gratitude journaling, engage in deep work practices, drastically limit social media and the news, and follow a number of other strategies aimed at promoting well-being and good mental health. I discuss them in more detail here.
Am I worried about the consequences?
As may be evident by now, I do apply pharmacology to many areas of my life. To me, pharmacology is one of the most interesting sciences because it is one of the few things that are akin to a “superpower”. However, in order to apply it in a way that the benefits outweigh the risks, it requires a deep, well-principled understanding of a host of other medicine-related sciences such as physiology, biochemistry, neuroscience, and endocrinology.
As mentioned in the section on guiding principles, the modern world is an unnatural minefield and not very conducive to my general and mental health. Therefore, in my opinion, living in the modern world is just as unnatural as using pharmaceuticals to better navigate it.
Some of my friends & family believe that what I do is dangerous. According to my understanding of things, everything I do is much less dangerous than, for example, obesity, alcoholism, or smoking, which combined probably affect 50% of people worldwide. The only difference is that obesity, alcoholism, or smoking seem natural to most people because they are so common (“familiarity principle”).
Whether I can (and want) to keep all this up for decades, I do not know. It could be that unforeseen side effects arise, or that one or multiple of these is far riskier than I currently assume. Regardless, I would rather opt for a below-average lifespan while feeling great and enjoying my time instead of living for very long but feeling mediocre.
Also, I simply do not know how long the world as I know it will still exist. While the chances that humanity becomes something far greater in the 21st century are high, the chances we screw up or that something escapes our control are high as well, such as climate change, engineered pandemics, artificial intelligence, technological singularity, or a catastrophic war. In the case the world falls apart within the next few decades or so, I believe that I have made a good deal.
I discuss some of my philosophy in more detail here.
Ranking
What follows is my personal ranking of the interventions discussed in this article. I am n=1 and what works for me, does not necessarily work for others. Furthermore, we are all different in terms of our neurobiology and what we want out of life.
Edit 12/24: I made this ranking back in 2023. Given that my “stack” has now changed quite a bit (see below), this ranking is not up to date.

Because each of the following has its individual usefulness, I found it nearly impossible to rank the molecules discussed. However, if I had to pick, I would pick in the following order. Of note, while I have experimented with all of the below, I do not currently take all of them.
- #0 – Human connection & finding purpose: Without emotional or “spiritual” health, feeling good and performing well does not matter.
- #1 – Sleep hacks: With regularity, darkness, ear plugs, a morning daylight lamp, glycine, magnesium, and a Chili Pad in the summer, I have a refreshing sleep on most nights, which has far-reaching effects on everything I do, think and feel.
- #2 – Exercise: Other than high-quality sleep, there is little that has a greater effect on my vitality than consistent, high-quality exercise, especially cardiovascular exercise.
- #3 – My TRT Lite Program: Benefits I have noticed include more energy, slightly less need for sleep, greater emotional intensity, an easier ability to build muscle, and a higher libido.
- #4 – Semaglutide & increasing caloric intake: I find hunger distracting and semaglutide is a potent appetite suppressant. For me, the increase in productivity and well-being can hardly be overstated. I should note that I do not use semaglutide to lose weight but rather to decouple my caloric intake from my appetite. I eat the highest possible number of calories that does not result in fat gain, which made an enormous difference to my vitality. Of note, while increasing my caloric intake may be great for my vitality, it is probably not optimal for longevity. However, vitality is more important to me.
- #5 – Moclobemide: While I was on it, moclobemide was a great all-in-one solution for energy levels, mood, and all while feeling natural and having few to no side effects. The downsides included a very slight cognitive and emotional blunting.
- #6 – Psilocybin: Friends use it occasionally to enjoy a day off, or to get some “deathbed” clarity in their life.
- #7 – Ketamine: Ketamine is very effective at reversing the neurobiological aspects of depression. It is perhaps the only antidepressant that enhances emotions instead of blunting them. Other than being hard to get hold of, the major downside is that it is potentially neurotoxic.
- #8 – Bupropion: Bupropion is a milder but more sustainable derivative of amphetamine. It is an effective mood brightener, stimulant, antidepressant, ADHD medication, weight loss drug, and anti-addiction agent.
- #9 – Vortioxetine: As I was taking it, it boosted my mood, energy levels, stress resilience, and cognition while having a very benign side effect profile.
- #10 – Nicotine gum: I find nicotine gum useful for increasing task salience and for boosting executive functions while working on cognitively demanding tasks. I can also take it at night without it affecting my sleep.
- #11 – Modafinil: A great stimulant to take occasionally. It lasts all day. However, as with all stimulants, the price is counterregulation, worsening of sleep, a change in personality, and doing things more thoroughly than intended.
- #12 – Rapamycin: Unfortunately, vitality and longevity are sometimes at odds. For example, the most rapid period of aging we go through (puberty) is also the period when vitality is usually greatest. While not directly helping with vitality in the short term, rapamycin helps to preserve vitality in the long term. According to the currently available data, rapamycin is presumably the most potent geroprotective molecule currently available to mankind. I have been on it for a little over four years.
Edit: Update on 12/2024 – What has changed in 2024?
I wrote this article in 2023. Since then, a couple of things have changed. While I try my best to update this article regularly, I decided against rewriting the section above to give readers a sense of how things are evolving over time. The things listed below have been a stable part of my protocol for at least six months.
- By far the #1 thing for my vitality is having an amazing group of friends and spending much of my free time with people I value. Furthermore, having purpose and a fairly set direction in my life is also having a big top-down effect on my physiology and neurobiochemistry. I mentioned this already but it is worth mentioning again because it is probably mostly read over because it sounds so cliché – but it is true!
- After having been on a low dose of semaglutide for 3 years, half a year ago I came off it. I am currently trying to gain weight, which semaglutide makes impossible to do. Interestingly, for some reason, my appetite is now much lower than before the semaglutide, hinting at the possibility that all this time on semaglutide led to some favorable rewiring of my appetite centers. However, I also gained weight which is a huge confounder.
- I realized that on moclobemide my IQ is roughly 10 points lower, which made me stop it. I still recommend it to friends, and for most people, it does not seem to affect cognition.
- For the past 10 months, I have been on “TRT lite”. Essentially, I take 100 IU of HCG per day. On this dose, my T levels are around 1000ng/dl, my E2 is at around 40pg/ml, and I am not even shut down (i.e., my LH and FSH are still within the low normal range). I describe my first run with TRT here. Last year I gave TRT another go and quite liked it, presumably because many other things were fixed that had not been fixed during my first try. I then switched over to my “TRT lite” protocol, which achieves the same thing but without the risk of a prolonged shutdown. My energy levels are higher, I need less sleep, my libido is greater, and I just generally feel well. In-depth article here: My TRT Lite Protocol. In order to not virilize too much from the increased androgen exposure and to age “more gracefully” I take a low dose of finasteride (0.125mg/d) along with it. Background: Individuals with hypogonadism look much younger than they are vs. people on TRT (after a couple of years) usually look much older than they are as they seem to age considerably faster than normal. Only temporary side effects from the finasteride. In-depth article: My Experience With Low-Dose Finasteride to Lock In My Prime
- Whenever I have a hard time falling asleep, I still take a low dose of triazolam sublingually (as I did before). I do this about once per week to once every other week or so. There has not been an increase in frequency or dosage over the past couple of years. Article here.
- From time to time, I struggle with anhedonic depression. This happens about 3-5x per year lasting a couple of weeks. I had been dealing with this for years now. During these episodes, I do all the things I normally do (e.g., work, gym, friends) but I feel quite little. The weird thing is that from the outside nobody can tell. When I tell friends that during these times I actually feel quite a little, they usually do have a hard time believing me because I am laughing, making jokes, and seeming emotional just like always. I am not even acting or putting up a facade. I also am not dissociated as far as I can tell. There is just a mismatch between what I do and what I feel. Even my psychotherapist does not believe me (“A person that feels little is not acting and talking the way you do.”). However, on the inside, there is emptiness. It is quite hard to explain. Also, these episodes seem to have very little effect on my “objective” life. I still go for walks, reading, dating, and my drive is unaffected. However, I do all of these things without “feeling” much. Other than the anhedonia, I am also more fatigued. I am quite unsure whether the cause is mostly biological or mostly “psychological”. My intuition tells me that during these times neuroplasticity is at low levels as everything that is known to have neuroplastic effects brings back my feelings (at least by a bit). However, pathogenesis is not the same as etiology. Anyway, a single dose of ketamine has thus far always been sufficient to kick me out of it. I am always reluctant for a couple of weeks to use it because it is probably more neurotoxic than the medical community currently appreciates. If the “waiting it out” does not work, 24 hours after the ketamine self-injection, it seems as if somebody has turned my feelings back on and usually they remain on for at least a few weeks, sometimes months. I aim to not use it more often than once a quarter (ideally, less). Recently, I also found NSI-189 very valuable in terms of getting out of this state but it needs more testing. Since gaining weight (both body fat as well as muscle) I seem to get these episodes less but again here, I am not very sure. Will update next year.
- I switched out the Huel for kefir yogurt drinks, which I mix with 70ml of olive oil + 1 whey shake – totaling 900 kcal per drink. I usually drink 2-3 of these next to my normal meals. I also noticed that I feel better if I eat less clean (still far away from fast food/junk). Because I am lean and fit, I can tolerate a much less clean diet – in fact, I feel much better when I am less strict with my food choices.
- This year I purposely gained weight. I tried to gain 1kg per month, starting in March. Overall, I gained 7kg, probably half fat and half muscle. My body fat went from 9-10% to roughly 13-14%. Since gaining weight, I have not gotten sick a single time (despite working in emergency medicine during this time). Furthermore, my energy is considerably higher, which is worth a lot to me. Also, I only got one single anhedonic episode, though it is hard to infer causality. Overall, I just feel better at slightly higher body fat levels and metreleptin can only partially hack this.
- My favorite stimulant has become yohimbine and, with very few exceptions (e.g., some modafinil during particularly brutal night shifts), the only stimulant I used over the past half a year or so. Whenever I need a push, I take 1.25mg of it. I am a homozygous CYP2D6 poor metabolizer so for me the yohimbine lasts considerably longer than for normal metabolizers. I feel stimulated by the yohimbine for roughly 4-6 hours. Just very clean energy. Yohimbine is an alpha2-antagonist and basically “disinhibits” noradrenergic tone (sympathetic nervous system activity). For me, yohimibine is the perfect caffeine replacement. It has barely any tolerance, no comedown, and does not mess with my sleep. For some reason, most people seem to dislike yohimbine – we are all different. Article on yohimbine here.
- In terms of recreational drugs, once a month to once every other month I take a low dose of plant medicine (0.5-1g) to have “a month’s worth of psychotherapy in one afternoon”. Occasionally, at parties I also take a low dose of 1,4-butanediol – great replacement for ethanol, which I never to rarely (once per year) drink. No deleterious effect on sleep and no hangover. About once per month.
- I am currently experimenting with pharmaceutical-grade NSI-189 and pitolisant. I have been only using them in cycles for a few months. Both are very interesting molecules. On NSI-189, which is a stimulator of neuroplasticity/neurogenesis, my dreams are very vivid and my libido is undeniably higher. I also seem to have more and deeper emotions. Pitolisant elevates central histamine levels and gives wakefulness without any stimulant effects (i.e., unlike modafinil and other stimulants). For me, both molecules have no side effects – at least none that I would have notied. My experience in more detail with pitolisant here and NSI-189 here.
- On and off I use a topical 17-beta estradiol cream for facial skin care (the same product postmenopausal women use for HRT – I just use a much smaller dosage).
- I limit my use of nicotine gum to 1 hour per day while I am reviewing notebooks from the past (e.g., science, thoughts, etc.). Nicotine is a powerful self-conditioning agent.
- I share updates regarding my protocol in my weekly newsletter. If you are interested you should sign up below.
- My longevity protocol has not changed too much.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
My Longevity Protocol
My current longevity protocol can be found here: My Longevity Protocol
Part II. Lifestyle
Most individuals are quite vital (to the point of being hypomaniacs) as little children. They have boundless energy, are motivated, curious, enthusiastic, capable of feeling profound feelings, and often have lofty dreams and goals. As people grow older, they typically experience a slow and steady decline in vitality, leading to a significantly reduced level of energy and vigor in their later years.

Next to poorly understood changes in central nervous system gene expression and neuroplasticity, vitality is first and foremost determined by general health, hormones, and neurotransmitters, which are to a large extent determined by my genetics and lifestyle.
I discuss the importance of genetics for vitality here.
I will now briefly discuss lifestyle factors, and I will also share a few insights and hacks that have benefitted me in the past. This part is the most important part of this article as it is concerned with what I call “baseline vitality”.
Hormones (Part III), nutrients & supplements (Part IV), antidepressants & related molecules (Part V), and stimulants (Part VI), will be discussed at later points in the article.
Unfortunately, lifestyle is something that doctors rarely talk about despite the medical literature clearly pointing in this direction. Needless to say, fixing diet, exercise, sleep, and hormones can radically transform someone’s physical and mental health.
A note on “gentle” enhancements
In part II (lifestyle) and part III (nutrients & supplements) of the article, I´ll mention many things that could be called “gentle enhancements” (the “big guns” are discussed in later parts of the article).
For example, whenever ambient temperatures are outside of my thermic comfort zone and warmer than I would like, I am, let’s say, 3% less patient, 7% more aggressive, and my mood goes down by 5% – usually without me being aware. Improving ambient temperature then has a significant but barely noticeable impact on the way I feel and function.
Similarly, gentle enhancements can yield small gains in certain aspects of vitality. For example, using blackout curtains, fixing vitamin B12 levels, exposing myself to bright light in the morning, changing macronutrient composition, etc. are all not game changers by themselves but at the end of the day, a 1-5% improvement in various domains is certainly not nothing.
And if a dozen or so of these low-hanging gentle enhancements are layered on top of each other, impressive improvements in vitality can be achieved, with compounding interest over time.
I discuss how gentle enhancements can lead to non-gentle results in more detail here.
Table of contents
Human connection
I am looking to be loved, to be appreciated, to matter. And a lot of things I think and do are probably rooted in this core desire, which is deeply ingrained in human biology and survival instincts.
Throughout our evolutionary history, a member of Homo sapiens left by itself was doomed to die since it did not have access to tribe-provided stuff such as food, shelter, warmth, protection, and mates. Everything related to its survival was found within and through the social domain, which is still true today.

Therefore, evolutionarily speaking, belonging to a tight-knit group and having deep connections with others was (and still is) of existential importance to humans. When a human being lacks it, the brain evolved to respond with feelings of distress (loneliness) in the same way it evolved to respond with feelings of hunger and thirst whenever there is a shortage of food or water.
Conversely, humans who are part of a community are rewarded with feelings of deep well-being in an analogous way evolution rewarded humans with short-term pleasure from sugar or sex.
In a similar way that hypothalamic cells measure energy intake and determine appetite vs. satiety (POMC neurons), new research suggests that there is something similar for regulating “social satiety”, including “rebound socialization” after prolonged social isolation in rats.
This has been proven in rodent species and a certain group of hypothalamic neurons responsible for regulating social behaviors (MPV neurons) has been identified. These neurons are intimately connected to oxytocin and vasopressin neurons.
In the human brain in particular, large parts of the brain are specifically designed for dealing with social stimuli, hierarchy negotiation, status concerns, and keeping score of social relations.
Unfortunately, today’s society doesn’t facilitate the same kind of camaraderie and sense of community that humans are likely wired to require. The recent rise of individualism with a focus on status and self-esteem surely did not help. This has left many people feeling empty and lonely.
From the available research it seems that having high-quality social ties is associated with better health and a longer life expectancy – though admittedly the effect is probably not as direct as it may seem due to possible confounders being at play such as healthy and vital individuals being more likely to have high-quality connections.
Regardless of putative effects on health and lifespan, having high-quality relationships is an important factor for mental health and well-being, probably even exceeding exercise or sleep. Said another way, individuals with great human connections but “bad” sleep and exercise habits may be happier than individuals with poor human connections but otherwise “great” lifestyle habits.
As Mark Manson expresses it: “And just like a beaver must build a dam to truly express his beaverness, humans must form social bonds to fully express our humanity.” Or as Johann Hari puts it, just like bees evolved to live in a hive, we humans evolved to live in a tribe. If we disband our tribes, we pay a price.
Personal experience
In my early twenties, I used to be quite introverted and prone to spending most of my time on “my things”. Over the last couple of years, I was fortunate enough to find my tribe of people who I can connect with in a deep and genuine way.
Having found my community is one of my biggest sources of fulfillment and has improved my life, productivity, and happiness in ways that are difficult to overstate. In a way, I would call it my most important “biohack”.
A note on status
Related to connection & belonging is the intrinsic human desire for status. This desire is highly biologically determined because, for millions of years, someone’s status in society determined preferential access to food, mates, and shelter. In fact, large areas of the human brain are dedicated to status & hierarchy negotiation, both of which are of essential importance for survival and reproductive success.
So, it is no surprise that a change in status would lead to a change in certain aspects of brain function. In fact, your (perceived) status in society has a strong influence on your neurotransmitters and neuroendocrine function (hormones). For example, in many primate societies (including humans), after males rise in ranks and become alpha males, testosterone and cortisol levels are known to rise. Similarly, depressed individuals often perceive themselves to be low status (and vice versa) – something known as the “rank order hypothesis of depression”.
A modern manifestation of this inherent drive for status is people’s desire to be “popular” on social media and the self-worth alterations by other people liking (or not liking) your content.
In this way, status (or the perception of one’s status) affects energy levels and mood through its effects on neurotransmission and neuroendocrine function.
Sources & further information
- Book: Sebastian Junger – Tribe – On Homecoming and Belonging
- Scientific review: The Neuroendocrinology of Social Isolation
- Video: Kurzgesagt – Why You Are Lonely and How to Make Friends
Purpose
After experimenting with all kinds of molecules, I found that, like human connection, purpose is the best antidepressant (reducing suffering & making me happy) as well as stimulant (giving me loads of energy & motivation) available.

Personal experience
Throughout most of my life, I had a sense of purpose and whenever I was lacking it, vitality enhancement, with a special focus on dopamine always seemed to increase my chances of finding it again. However, out of all of the things in this article, purpose is probably the hardest one to get.
Here I want to specifically mention psychedelics, which helped some of my friends a great deal in this regard. Next to having helped with getting unstuck in the egocentricity loop (“I am the center of the universe”), a friend who was gripped by a sense of meaninglessness came out of one session feeling part of something larger than himself. The effect catalyzed an upward spiral.
However, I also know people who were seriously harmed by psychedelics so they are best approached with the respect they deserve.
I discuss psychedelics in much more detail here.
Sources & further information
- Book: Viktor Frankl – A Man’s Search for Meaning
- Scientific opinion article: New Movement in Neuroscience: A Purpose-Driven Life
- Scientific review: Psychedelics and Psychedelic-Assisted Psychotherapy
Sleep
Getting a good night’s sleep is one of the best time investments I can make, as it gives me the energy and mental clarity needed to perform well in life. It also makes me more alert, energetic, motivated, creative, and happier.
Conversely, whenever I am sleep-deprived, I am more prone to distractions, worse at everything, and I enjoy things less. For me, bad sleep dwarfs the physiological and mental detriments I experience from a bad diet or no exercise.
During university, I have had extended periods of time during which I only slept for five to six hours per night. In retrospect, cutting down on sleep was a very unproductive thing to do. My performance was worse, and so was my metacognition. Furthermore, I was often working on the wrong things. Even when I was working on the right things, I was easily distracted. I was constantly semi-“drunk” and everything was hazy.
Now, my sleep is great, and improving it has been among the most fruitful things I ever did.

Sleep is necessary to “reset” the brain because there are a large number of cellular processes that can only be carried out during sleep. These include clearing out metabolic detritus, reregulating the expression of a large number of neuronal genes, executing hundreds of cellular housekeeping tasks, and synaptic regulation.
Therefore, without sufficient sleep, the nervous system is dysregulated. And my nervous system is responsible for many things I value.
Sleep is necessary (but not sufficient) for good pattern recognition, memory consolidation, metabolic integrity, hormonal health, executive functions, emotional control, focus, creativity, and life enjoyment.
Good sleep is also important for emotional stability. There is no mental illness in which sleep is normal – bidirectional causality. Furthermore, good sleep is crucial to willpower – which is crucial to everything else.
What follows are several strategies that have helped me to improve my sleep.
- Going to bed at the same time
- Early to bed, early to rise
- Pitch-black dark
- Quiet environment
- Cold temperature
- No alcohol
- Avoiding caffeine
- Avoiding large meals
- Eating carbs at night
- Morning blue light exposure
- Evening blue light exposure
- Supplements
- Melatonin
- Hypnotics (“sleeping pills”)
I will now briefly discuss each.
Going to bed at the same time (regularity)
I find that one of the best things I can do for better sleep is go to bed at the same time each day (+/- 30min). It’s not just the total hours of sleep each night that matters but also how my sleep time aligns with how my circadian rhythm is entrained, which changes the timing of sleep stages.
For example, if I go to bed later than usual, even by just one hour, my sleep quality is going to be worse, even if I sleep for the same amount of time. I feel less refreshed the next day, and I tend to procrastinate more. I believe that I am more sensitive to this than other people.
Early to bed, early to rise
My preferred sleep time is 22.00-06.00. Fortunately, I am naturally a morning lark and I do not have to fight my genetically influenced chronotype.
There seems to be evidence that under truly natural conditions, such as if electronics are taken away from people, most people have somewhat similar chronotypes and most prefer going to bed before 22.00. Most people also have better sleep quality if they go to bed earlier rather than later, even if total sleep time remains the same.
Pitch-black dark
I make sure that my bedroom is very dark (so dark that I can’t see anything basically). I find that even tiny amounts of light worsen my sleep even if I subjectively do not perceive the light as disturbing.
The human eye is very sensitive to even minute quantities of photons, and whenever the retina captures brightness, it sends signals to different regions in the brain stem’s reticular activating system, which then triggers small changes in the release of acetylcholine and noradrenaline, leading to decreased sleep quality and micro-awakenings.

Some people claim that they can sleep “just fine” in non-dark environments. However, “just fine” is far from optimal and I find that making my bedroom pitch-black dark is a simple but powerful hack with a high return on investment.
I use blackout curtains and have covered all electronic lights with black tape. I do not use a sleep mask because when I do, I always end up pulling it off during sleep.
Quiet environment
Similar things apply to sounds. The brain stem is quite sensitive to auditory input and certain sounds are known to disrupt sleep quality. Using earplugs has considerably improved my sleep quality. I use Mack’s silicone earplugs, which I also use for studying.

Cold temperature
I make sure that my room is fairly cold. Year-round I also use a cooling blanket made of 80% nylon and 20% polyethylene, which absorbs heat from my skin and conducts it away, dropping skin temperature by 2-5 C.
In the summer months, I use a Chili Pad, which significantly improves multiple aspects of my sleep, such as sleep latency (how long it takes me to fall asleep) and deep sleep.
Because it boosts my productivity for 3-4 months per year, I consider my Chili Pad to be one of the most lucrative investments I have ever made.
I have also tried the Ooler sleep system, which is a little bit “better” than the Chili Pad. One of the major advantages of the Ooler system is that it can be set to warm up in the morning. However, I can do the same by connecting my Chili Pad to a smart plug that automatically turns off at 5 am.
One friend of mine sleeps on an Eight Sleep mattress, which he loves, though it is pricy.
Avoiding caffeine
I rarely consume caffeine. Even if I drink a few sips of green tea at night, my sleep is affected. I have met a lot of people who believe that they can drink caffeine in the late afternoon without their sleep being impaired. According to scientific data, this is nonsense, and quite a considerable reduction in sleep quality can be detected by polysomnography (even for people who think that their sleep is not affected by it).
I discuss caffeine in more detail here.
Alcohol
One of the most detrimental effects of alcohol is its adverse effects on sleep.
The last time I drank a double shot of tequila (I rarely drink alcohol), my REM sleep and SWS numbers were crushed, my body temperature was higher, my heart rate variability among the lowest it had ever been, and my sleep tracker (Oura) readings for sleep and readiness score were abysmal. Objective data aligned well with my subjective experience.
Some of my friends use alcohol (or THC) to wind down at night, and even specifically to help with sleep onset. However, alcohol is known to worsen sleep in any aspect other than sleep latency (how long it takes to fall asleep). Furthermore, if consumed chronically, rebound insomnia is likely to occur after stopping which perpetuates a vicious cycle.
A note on sleep trackers
I love the Oura ring, though I have not tried other sleep trackers. For me, my Oura data usually matches my subjective perception of my sleep quality quite well.

A couple of my friends were on their way to run into “sleep-tracker-induced sleep disorders” because they are so neurotic about their metrics. More data is not always better, and for hypochondriacs, or people who are overly neurotic, sleep trackers may take more than they give.
Avoiding large meals before bed
Eating a small meal close to bedtime has a negligible effect on my subjective and objective sleep data. However, eating a large meal close to bedtime requires a lot of energy for digestive processes, which drives up heart rate & body temperature, reduces my heart rate variability (HRV), and has me waking up feeling groggy.
Below are two screenshots of my sleeping heart rate. The left is “normal”, and the right is after having eaten a big meal before bed. I find the change in deep sleep and REM numbers quite impressive.

A large meal before bed is also known to interfere with growth hormone secretion, the majority of which happens in the first third of the night.
Carbohydrates at night
Whenever I eat a reasonable amount of carbs at night, my sleep seems to improve. Conversely, when I do not eat any carbs at night, usually I find it hard to fall asleep. This is presumably due to insulin’s stimulatory effect on the serotonin system and inhibitory effect on the orexin system, two systems intricately tied to sleep regulation.
However, if I eat a lot of “bad” carbs too close to bedtime, I take much longer to reach deep sleep, and I feel a little groggy the next day even though my total sleep time tends to increase.
I discuss carbohydrates in more detail in the section on diet.
Exercise
Studies consistently find that exercise improves sleep quality, including total sleep time and increased slow-wave sleep. This aligns well with my personal experience.
If I go without exercising for a few days, my sleep quality declines. However, one downside of engaging in intense physical activity is that it raises my sleep requirements by approximately one hour.
Whenever I exercise too close to bedtime, I take much longer to fall asleep, and my heart rate and body temperature remain elevated for the first half of the night, preventing me from properly reaching deep sleep. This is likely caused by the uptick in metabolic rate and the microspike in cortisol levels. Taking a cold shower before going to bed seems to help a little.
I discuss exercise in more detail shortly.
Morning blue light exposure
After waking up, I use a 10.000lux daylight lamp as my desktop lamp. I believe that it does not really matter that much whether the light comes from the sun or a lamp as long as the cumulative light exposure, brightness, and wavelength are the same.
Because daylight brightness is obviously much brighter than artificial light I try to partially get around that by using my daylight lamp for about 2 hours. The daylight lamp I use is a Beurer TL41.
Right after waking up, I use light therapy glasses (Luminette 3) for about 15 minutes at the highest setting. The main benefits of this are twofold. Firstly, the glasses shine light directly into my retina at a decent intensity. Secondly, I expose myself to light while I am going about my morning routine (e.g., bathroom, getting dressed, stretching, etc.). Both of these things would not be possible with conventional daylight lamps.

A friend who is prone to winter depression and usually uses a microdose of escitalopram to deal with the seasonal dip in energy & mood. He claims that using Luminette 3 for 30 minutes per day triggers a “switch” for him that normal light therapy does not.
I try to expose myself to bright light throughout the day. For example, when I am working at home my daylight lamp is usually on for multiple hours. I also use my light-therapy glasses for about 15 minutes once in the afternoon.
In the short term, exposing oneself to bright light in the morning stimulates morning cortisol release (which is a good thing). Furthermore, through direct retino-raphe projections, it also elevates serotonin signaling. The increase in cortisol combined with an increase in serotonin transmission helps with my energy and mood for the coming day. Bright light in the morning is thought to also affect the dopaminergic system.
In the long run, regular exposure to bright light in the morning synchronizes my circadian rhythm, potentiates the cortisol awakening response (CAR), improves levels of various neurotransmitters, and improves body temperature patterns. These effects are sustained even if I stop exposing myself to bright light for a few days.
Evening blue light exposure
For me, moderate amounts of blue light at night have far less of an adverse impact on my sleep (both subjectively as well as according to Oura data) than what I had initially assumed. Though, as with everything, there are probably individual differences in evening blue light sensitivity and it is probably best to avoid it if one can do so comfortably.
Supplements
I take 400mg of non-oxide-form magnesium, 5g of glycine, and 500mg of taurine before bed. All of these make a small, but measurable difference to my sleep quality. I was specifically surprised by the power of glycine. I discuss all of these in more detail in the section on supplements.
Melatonin
Melatonin is a double-edged sword.
- On the one hand, melatonin drops core body temperature, entrains the circadian rhythm, helps with sleep onset and quality, and amplifies growth hormone release during sleep.
- On the other hand, melatonin also controls seasonality and hibernation, and it downregulates the secretion of “energy” hormones (thyroid hormones, sex hormones, stress hormones), particularly at higher doses.

It is thought that small doses of 0.3-0.5mg can be safely taken long-term. Melatonin is not just useful to entrain circadian rhythm, but it may also help with sleep onset & sleep quality because it is a hypothermic agent.
I currently do not use it because I feel that I have a strong Circadian rhythm already. Furthermore, the risks and downsides, especially concerning the endocrine system, may outweigh the benefits. Interestingly, whenever I start to take it, for the first couple of days I wake up very alert and full of energy at 4 am, presumably because my circadian rhythm has been “confused” by exposure to the artificial spike in melatonin levels. However, this seems to go away shortly.
A couple of friends use 0.5mg extended-release melatonin with good results.
Other hormones
Next to melatonin, multiple other hormones affect sleep. These include testosterone, estradiol, progesterone, thyroid hormones, growth hormone, IGF-1, leptin, insulin, and cortisol. I discuss some of these hormones in more detail here.
The older one gets, the less REM and SWS and the more stage 1 and 2 (shallow sleep) there are throughout the night. This is partly related to the decline in growth hormone. After I had put my dad on a short course of a low dose of growth hormone, he mentioned how amazing his sleep had become and how rested he felt after waking up. The increase in sleep quality is one of the most common observations after people try growth hormone therapy.
Sleep apnea
A friend of mine has sleep apnea. Because of that, he spends very little time in slow-wave-sleep (SWS). Before treatment, he was always tired, he needed over 9 hours of sleep to feel at least partly rested and had what is called “excessive daytime sleepiness” (EDS). Getting a CPAP device and a device called “Velumount” significantly helped him, and so did losing body fat.
Sleep apnea is a serious condition that can strip years from a person’s life if left untreated. About 80% of people who have sleep apnea are currently undiagnosed, and sufferers are frequently not even realizing that they are waking up a ton, vacillating between non-REM light sleep and brief semi-conscious wake-ups, which prevent people to enter restorative deep sleep, eventually decreasing health, longevity, and well-being on a variety of dimensions.
Checking for sleep apnea is ideally done in a sleep lab.
Meditation
A couple of friends find meditation before bed particularly helpful when they are stressed out and their mind is racing. I personally can’t meditate at night, simply because I am not alert and “present” enough. I discuss my experience with meditation in more detail here.
Hypnotics (“sleeping pills)
I have experimented with all kinds of sleeping pills, and occasionally, I still use two of them. Because sleep drugs are technically not lifestyle interventions, I discuss them separately here: Hypnotics (“Sleeping Pills”).

Single-night sleep deprivation
I include this just because I find it interesting. I find that sleeping very little for a single night has potent stimulating effects on me, presumably as it boosts glutamate, dopamine, and cortisol levels.
Because of this, sleep deprivation is sometimes employed therapeutically to treat depression. Unfortunately, the stimulant and antidepressant effects do not last very long and are often paid for with a crash.
Sleep is necessary but not sufficient for feeling rested
I discuss other common (but often overlooked) causes of fatigue in more detail here: “I Am Tired All The Time” – 12 Overlooked Causes Of Fatigue
Sources & further information
- Scientific study: Light therapy in non-seasonal depression: An update meta-analysis
- Book: Matthew Walker: Why We Sleep
- Podcast: Huberman Lab Podcast: Master your sleep & Tools for optimizing sleep
Exercise
As with sleep, the time invested in exercise has a high ROI on a number of domains, including my health, energy, mood, creativity, sleep, looks, and happiness. Furthermore, exercise is among the healthiest things I can do for my brain. In this section, I will discuss the effects of exercise on vitality and not so much on other health-related aspects.
There is a neurobiochemical reason for the saying “You are only one workout away from a good mood.”.
- Firstly, during intense exercise, the “nasty” kappa-opioid system in the nucleus accumbens shell (the brain’s major hedonic hotspot) is activated, which mediates the subjective experience of discomfort. However, as a counterregulatory mechanism, the “feel-good” mu-opioid system is activated and remains activated for a couple of hours after
- Secondly, exercise boosts noradrenaline and cortisol, both of which increase central nervous system “readiness” for a couple of hours.
- Thirdly, exercise increases serotonin transmission for many hours to come. Whenever vertebrates exert themselves intensely, serotonin levels rise, in part to signal to the animal “Hey, chill down.” This prolonged rise in serotonin, which presumably serves self-protective purposes, is another main reason intense exercise makes me feel good for the entire day.
These neurotransmitters are discussed in more detail here: An Introduction to Neurotransmitters
Exercise makes me feel and function so well that I would even do it if it did not have any other beneficial long-term effects – which it undoubtedly has.

I particularly appreciate its beneficial effects on both short-term brain function as well as long-term brain health. My nervous system is the basis of everything I think, do, and feel, and few things improve it as much as regular exercise.
- Exercise stimulates the release of nerve growth factors such as BDNF & VEGF. In fact, it seems to be one of the most neurogenetic interventions available to mankind – endurance exercise more so than resistance training.
- Regular vigorous exercise promotes cell proliferation in the hippocampus, which enhances mood, memory, and cognition. In part because of this, exercise is probably among the most powerful tools I have to stave off cognitive decline.
- Exercise stimulates the locus coeruleus, the brain’s major source of noradrenaline, and causes this collection of cells to increase in size and baseline activity. Therefore, over time, exercise really does lead to a more alert brain and the reason is a long-term structural change (or better, a combination of multiple structural changes).
- Exercise increases brain oxygenation and improves sleep, both of which are crucial to brain health.
Through the combination of these short-term and long-term effects on the brain, exercising regularly improves energy levels, mood, and cognition, and also slows the rate of neurocognitive decline.
There are all sorts of other reasons (beyond brain health) why exercise is powerful beyond belief. Exercise improves sleep, hormones, insulin regulation, nutrient partitioning, and musculoskeletal health. Exercise is also one of the most potent interventions available to slow neurocognitive decline.
Regular vigorous exercise also causes hundreds of changes in gene expression, affecting almost any level of physiology, biochemistry, metabolism, and health.
While some effects of the different kinds of exercise are overlapping (e.g., brain health, improving metabolic health, well-being), different kinds of exercise have non-overlapping individual effects as well.
For example, high-intensity exercise or HIIT induces antioxidant systems more than other forms of exercise, aerobic cardiovascular exercise has powerful effects on mitochondrial health and density. Low-intensity endurance exercise improves mitochondrial number and function. Low-rep range heavy resistance training particularly improves myofibrillar density and contractility. High-rep range resistance training leads to an increase in sarcoplasmic muscle growth and a host of metabolic adaptations.
Exercise is undoubtedly among the best tools available for delaying the inevitable deterioration of the body (“aging”) and extending health span and lifespan – perhaps even more powerful than rapamycin.
If family or friends ask me about the single most important thing they can do to improve their health and vitality, my answer is always the same: sleep & exercise. Of note, the exercise recommendations by official health agencies are pathetically insufficient for it to have the vast benefits it could have.
My exercise regimen
I exercise for about one hour per day. Whenever I do not exercise, I feel that something is missing. And if I do not exercise for multiple days in a row, I get antsy, irritable, and my energy and mood drop noticeably.
I do about 1h of exercise per day and I rarely take days off. I usually alternate between 60 minutes of steady-state cardio (in the form of zone-II exercise) on a recumbent exercise bike and the gym (alternating lower and upper body workouts). Twice per week I also do dedicated mobility training.
I specifically want to mention zone II exercise (long cardiovascular exercise sessions at the cusp of lactate threshold).
Zone II exercise is thought to be particularly powerful for improving mitochondrial health, function, and number. These better mitochondria then benefit people 24/7, including for cognitive tasks such as thinking or studying. This is presumably the reason professional chess players put a prime on cardiovascular fitness.
Below is a screenshot from my Polar data of what a zone II session looks like for me (I usually end with a 5-minute high-intensity part). My average heart rate is between 70-80% of my maximum heart rate (which is a little over 190bpm).

Whenever I am at home, I set a repeating alarm every two hours to incorporate “exercise snacks” into my day. These 2-minute-long bouts of exercise help me with alertness & cognition. I usually do 75-100 kettlebell swings, which are great for spiking my heart rate and working my posterior chain, both of which are well suited to counter some of the negative consequences of prolonged sitting.

I discuss my approach to musculoskeletal health and my exercise routine in more technical detail here.
Sources & further information
- Podcast: Peter Attia (The Drive): Exercise, VO2 max, and longevity
- Scientific review: Muscle–Organ Crosstalk: The Emerging Roles of Myokines
- Scientific review: Exercise effects on depression: Possible neural mechanisms
Heat & cold exposure
Cold showers
A couple of years ago, I was heavily addicted to cold showers. I would take an average of five cold showers per day for many months, each about 1-2 min long. I mostly “abused” them for their stimulant properties, and for the year or so I was doing them excessively, they essentially replaced stimulants.
I loved the mental clarity, the pick-me-up effect, and the alertness they provided. An even greater benefit was winning many small battles against myself many times per day, which built a lot of self-respect and self-discipline.

However, after a couple of months, I noticed two issues: Excessive vasoconstriction and a reduced ability to sweat. I discuss them briefly here: Long-term Side Effects from an Addiction to Cold Showers
I still love taking a cold shower and I take all my showers cold as they invigorate my body and mind for about 1-2 hours. However, I make sure not to do it more than once per day. Just as with most other things, moderation is best. Other putative benefits of cold showers include modulation of the immune system, activation of brown adipose tissue, and beneficial effects on mood (presumably due to their effect on catecholamine levels).
In my opinion, most of these non-immediate benefits (other than the mood benefits) are overblown and/or effect sizes too small to matter beyond the realm of statistical significance, though, I could be wrong.
Sauna
Sauna use is a great way for people to get some of the benefits of exercise without actually exercising. These include a variety of cardiovascular benefits such as an elevation of heart rate, whole-body vasodilation, and a temporary spike in cardiac output. With repeated use, heart rate variability improves, blood pressure goes down, cardiovascular health improves, and all-cause mortality decreases.
Furthermore, and just like exercise, sauna use is thought to also have a couple of neurobiological benefits such as inducing a release in growth hormone, a spike in brain growth factor levels, and a temporary boost in opioid and serotonin signaling. Some friends tell me that using a sauna at night also improves their sleep.

Uniquely, and unlike exercise, sauna elevates levels of certain heat-shock proteins, though the real-world relevance of this is debated.
If a sauna were easily accessible to me, I would use it more often. However, at present, I would have to make a special effort to use one. Furthermore, since zone two exercise (steady-state cardio at a heart rate of about 180 minus age) is likely to provide similar or even more benefits, the opportunity cost makes the prospect of using a sauna less appealing.
In my opinion, the benefits of sauna use are dwarfed by the benefits of an equal time spent doing zone two exercise, though, for most people, sauna use is more enjoyable in part because they do not have to “do” anything – just sitting back and enjoying the ride.
Sources & further info
- Scientific article: The Effect of Cold Exposure on Cognitive Performance in Healthy Adults: A Systematic Review
- Scientific article: The Cardiometabolic Health Benefits of Sauna Exposure in Individuals with High-Stress Occupations. A Mechanistic Review
- Scientific article: Changes in thermal homeostasis in humans due to repeated cold water immersions
Diet
When it comes to diet, many people believe that they have it all figured out but everyone else got it all wrong. However, diet science is an absolute mess and everyone can “disprove” almost anything everyone else says by cherry-picking from the available literature.

It seems that a lot of people got stuck on “nutrition absolutes” and miss the “it depends” part. The “optimal” diet almost certainly differs depending on several factors, such as activity levels, metabolic health status, body fat percentage, hormones, and genetics.
In an ideal world, people would be able to do their own research, but unfortunately, some of the research done in medicine, and especially in nutrition medicine, is inherently flawed due to bad study design, bad data-gathering practices, bad semi-objective measurements, confounded observations, using statistics in ways that amount to lying, or financial incentives.
Furthermore, like research about what kind of psychotherapy is most effective, a lot of nutrition science seems to mostly corroborate the previously held “conclusion” of the authors.
Below is a list of things I found work for me, some of the things I did in the past, and some comments on a couple of things some of my friends are doing. As with everything else on this blog, most of this is n=1, so it is best to be taken with a grain of salt.
- 80/20 principle
- Macronutrients
- Fats
- Carbohydrates
- Processed foods
- Sugar
- Variety
- Caloric intake
- Body fat
- Water intake
- Food intolerances
- “Superfoods”
- Thoughts on veganism
- Thoughts on intermittent fasting
- Thoughts on the ketogenic diet
- My experience with multi-day fasting
- Thoughts on the carnivore diet
80/20 principle
In my early twenties, I tried to be a diet perfectionist, which caused a lot of unnecessary stress and took away from life enjoyment. I now try to adhere to a good diet about 80% of the time, and for the rest of the time, I care little. I believe that occasionally eating junk if I need or want to, is not that big of a deal if my staple foods (the foods I eat 80% of the time) are good.
Macronutrients
There are few more polarizing diet topics out there than whether carbs or fats are good or bad. As with so many other things, it depends on the context.
Under normal circumstances (about one hour of exercise per day; 10-12% body fat), my preferred macronutrient composition is about 250g carbs, 250g fats, and 150g protein, though I am quite lenient with switching up carbs and fats, depending on whether I eat by myself or with friends. I also make sure to consume enough fiber (I particularly like the beta-glucans found in oats).
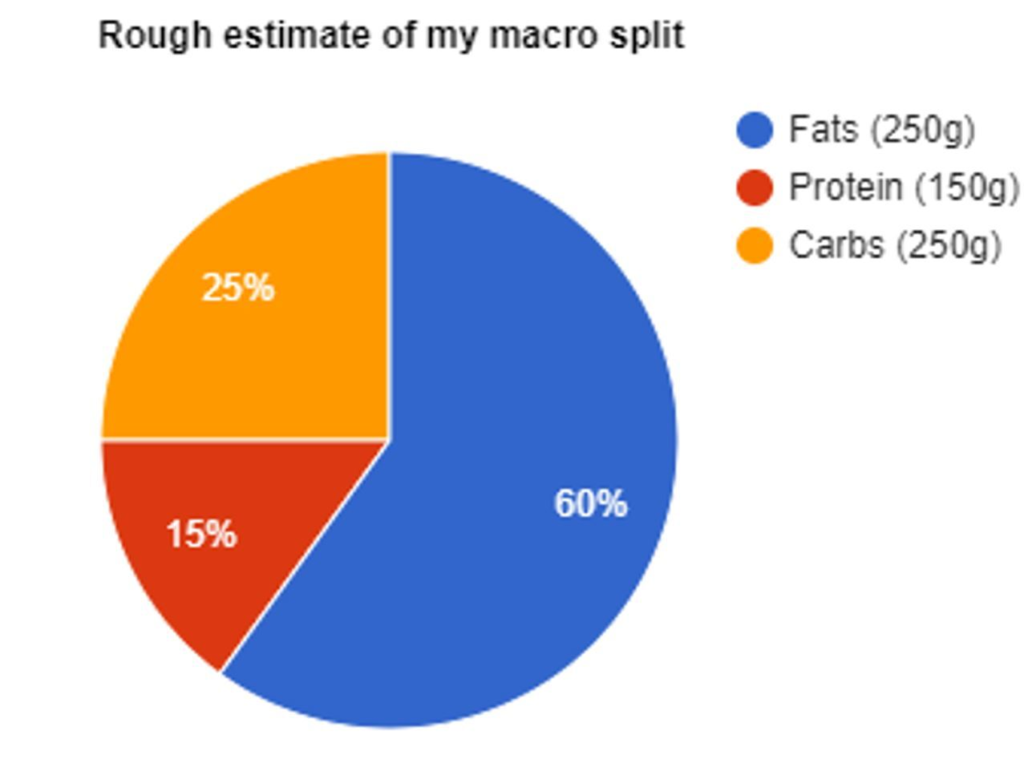
Fats
My preferred fat choices are monounsaturated fats (“good” fats) > saturated fats > polyunsaturated fats (mostly vegetable oils other than olive oil). I also aim to get about 2g of EPA/DHA per day (discussed in more detail in the section on supplements).
I usually go through two liters of olive oil per week (about 300ml per day). Olive oil is extraordinarily rich in monounsaturated fats, and it seems that almost everyone does well on monounsaturated fats, whereas some people react badly to saturated fats (in terms of their lipid profile), whereas others claim to react badly to polyunsaturated fats.
Carbohydrates
I titrate my carb intake to leanness and activity levels. Whenever I am very lean and/or highly active, reducing carbs is a bad idea. When I am less lean or less active, I try to reduce carbs and increase fats. However, I almost never reduce carb intake below 150g or so because I consistently feel and perform worse when I do.
My preferred carb choices are slow-releasing complex carbohydrates, such as oats. Whenever I eat a lot of fast-spiking refined carbohydrates (“bad carbs”) my cognitive function & alertness decline for a couple of hours unless I have exercised beforehand (after a hard workout, a lot of the ingested glucose is partitioned to my glycogen-depleted liver and muscle tissue). Therefore, I try to eat “bad carbs” predominantly in the evening or after heavy exercise.
Because I am lean, active, and pharmacologically hack my metabolism, I am quite insulin sensitive. Therefore, I can tolerate carbs very well and my body can dispose of them adequately by burning them or shuttling them into glycogen synthesis.
Conversely, if my glycogen stores were always tapped out (e.g., with a sedentary lifestyle), excess glucose is biochemically much harder to manage and comes with a host of unfavorable biochemical alterations.
When it comes to carbs, there is no “one size fits all”. An individual’s carbohydrate tolerance can vary quite a lot and depends on a number of genetic factors (e.g., variants in the PPAR-family of transcription factors), hormonal factors (e.g., IGF-1, thyroid hormones, sex hormones, AUC-levels of cortisol, leptin, adiponectin), insulin sensitivity, and activity levels.
Interestingly, pretty much all the high-energy people I know eat a diet rather high in carbs, including some fast-spiking carbs (“bad carbs”). I personally have also seen large benefits in terms of energy levels since increasing my carb intake. While I did have some temporary lethargy, it seems that in the long run, my baseline energy has increased.
Nonetheless, I believe that a low-carb, high-fat diet is great for people who are mostly sedentary, overweight, or insulin resistant. I will discuss my thoughts on ketogenic diets in more detail shortly.
A couple of years ago, I was occasionally using the drug acarbose, a glucosidase inhibitor, which “converts” fast-spiking (“bad”) carbohydrates into slow-release (“good”) carbohydrates. I did this to mitigate the negative effects of high-glycemic meals (e.g., at social gatherings when avoiding junk food is a nuisance). Unfortunately, even microdoses consistently spiked my liver enzymes.
There seems to be something harmful about large glucose spikes and they seem to be associated with all kinds of bad long-term consequences, including a reduction in lifespan. Some researchers speculate that large glucose spikes trigger something “bad” within the hypothalamus. Of note, the lifespan benefits of canagliflozin (an SGLT-2 inhibitor) or acarbose (a glucosidase inhibitor) likely come down to, at least in part, a blunting of peak glucose levels. I discuss my experience with metabolic drugs in more detail here: Metabolic Drugs.
I discuss acarbose, and several other metabolic drugs, in more detail here: Metabolic Drugs.
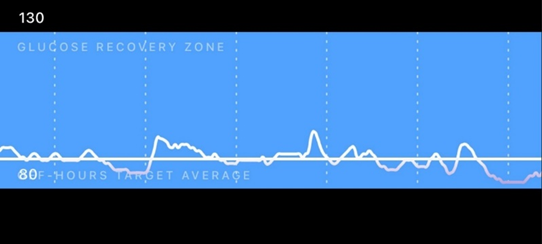
Processed foods
I avoid overly processed foods when I am eating by myself, but I do not care about it too much in a social setting (80/20 rule).
Processed foods have several things wrong with them: A lot of sugar and salt, a lack of fiber, excessive amounts of omega-6 fatty acids, a lot of additives, and usually a high caloric density.
Sugar
Like processed foods, I avoid sugar when I am eating by myself (but not socially) because I find sweetness per se to be addictive. Fructose is not only addictive and hunger-dysregulating, but the specific metabolism of fructose has a variety of detrimental effects on metabolic health, which I care about. I discuss sugar, fructose metabolism, and artificial sweeteners in more detail here.
Variety
I do not eat a varied diet and I also do not think that variety is essential. In my opinion “Eat a varied diet.” is only useful advice if my intake of micronutrients (vitamins & minerals) were poor. After I have found what works for me, I prefer eating the same things over and over again. Every other mammal out there does this.
The diet in “blue zones”, areas with the longest human life expectancy on Earth, is rarely varied. Yet, on average, blue-zone people live to a comparatively very old age and are in comparatively excellent health.
Caloric intake
It is not just about what I eat but also about how much. In my opinion, the total amount of calories is one of the most important factors when it comes to diet. From an energetic point of view, everything I eat becomes electron-donors and, according to the deepest principles of physics, my body can just give out what I put in – at least in the long run.
In the past, my obsession with “fitness” caused me to undereat for a lengthy period of time. For years, I was trying to survive on 2200-2400 kcal/d because online calculators aimed at figuring out my TDEE “determined” so. Furthermore, I was also reckless with intermittent fasting & ketogenic diets (more on that shortly).
After gradually increasing my caloric intake by about 1000 kcal/d, I started to feel much more alive, and my energy levels and mood increased significantly. Increasing my caloric intake was one of the best things I ever did for my energy levels.
Interestingly, despite eating vastly more, my body fat percentage remained about the same. I guess I fall into the high non-exercise-induced-thermogenesis (NEAT) category and if I eat more a number of hormones increase and I subconsciously raise my activity levels.
I find that the caloric intake I feel and function best at is the highest tolerated number of calories that does not result in fat gain. For me, that is around 3500-3800 kcal/d. Whenever I eat less than 3000kcal for a couple of days, my vitality decreases considerably, especially if I also do heavy exercise.
By far the greatest determinant of how much I burn is my basal metabolic rate (BMR). My BMR primarily depends on three things:
- Speed of metabolism: The speed of metabolism is mostly determined by a variety of hormones, in particular thyroid hormones. Because I supplement with thyroid hormones, my BMR is a little higher than it would be otherwise.
- Muscle mass: This is the speed of metabolism applied to muscle tissue. I have a decent amount of muscle tissue, which burns calories even if I just sit around, and much more if I exercise.
- Sympathetic nervous system activity: It is thought that differences in sympathetic nervous system activity are the biggest factor explaining different BMRs of people with the same weight and body composition. How strongly active a sympathetic nervous system is depends on genetics, hormones, stress level, stimulants (of which I mostly use nicotine), and ambient temperature. I guesstimate that my consumption of nicotine gum increases my BMR by about 150-250 kcal per day. I also prefer to work in a cold environment because I feel that it increases my alertness and cognition. Because of these factors, my sympathetic nervous system activity is (presumably) fairly high and requires a lot of energy to maintain.
I discuss why a “calorie” is not a “calorie” in more detail here: Why Weight Loss is not About “Calories In vs. Calories Out”
Body fat
I care about being lean because it makes me look much better overall. Because we humans are deeply visual creatures this helps me in a number of domains in life, not just dating. For me, the difference between being 10% body fat and 15% body fat is night and day, particularly in my face.
Furthermore, being lean is one of the best things I can do for my metabolic health and insulin sensitivity.
I usually hover in the 10-12% range (as measured by DEXA scans I do twice per year). In the pictures below I was at 10.6% body fat.

Hopping on semaglutide allowed me to keep my body fat fairly low without almost any effort. In fact, I need to watch my calories closely so that I do not undereat. Whenever my body fat gets below 10%, I feel and function progressively worse, regardless of whether I am on semaglutide or not. My energy, mood, libido, concentration, and vitality take a severe hit. I discuss this in more detail in the section on leptin.

It seems that most males feel and function best somewhere between 13-18% body fat, whereas most females feel and function best between 21-26%, though there is some interindividual variation.
Body fat is highly sensitive to genetics. There are a ton of people who do “everything right” but their body fat will hardly go below 15%. Conversely, there are others who can eat whatever they want and they are constantly under 10%. Next to hormonal factors, there are many other genetic factors, such as the amount of uncoupling protein (UCP1) expression.
Water intake
Even mild dehydration affects my energy, mood, attention, and cognition. I know that I am dehydrated when my voice starts to sound weaker and breathy.
I try to drink about 3l of water per day but not more than that (other than on days with excessive exercise or heat). Drinking too much water can wash out the medullary concentration gradient in the kidneys necessary for concentrating urine, which promotes polydipsia and electrolyte disturbances.
I use the color of my urine as a guide to how much water I should drink. While opinions different, in my opinion, slightly yellow urine is better than colorless urine.
I do not use water filters because the water in my city & house is naturally of decent quality.
Food intolerances
Figuring out whether I have an intolerance to a certain food is worth a lot.
- Eggs: I react badly to eggs but only if I eat them often. After two weeks or so of regularly eating eggs, I get tired and sluggish after eating them. This may be due to an immunological reaction against certain protein epitopes found in egg white.
- Dairy: One of my friends reacts badly to dairy, and after consuming it he feels lethargic for a couple of hours. This could be due to an immunological sensitivity to the alpha-s2-casein fraction, which actually seems to be quite common. I share my thoughts on dairy in more detail here.
- Nuts: It seems that quite a few people have immunological reactions to certain kinds of nuts, particularly cashews and peanuts, both of which are technically not nuts. Antibody development can be avoided, and existing antibodies reduced, by rotating different nuts.
- Grains: My aunt recently asked me about my thoughts on grains. Most people who claim to be immunologically intolerant to grains can likely tolerate grains just fine. The whole “gluten-free” thing is, in my opinion, mostly a marketing scam. Though I am open to updating my current stance.
I have researched insensitivity tests (somewhat) thoroughly and it seems that apart from lactose intolerance and celiac disease (gluten), there is no accurate, reliable, and validated test to identify food intolerances. Even tests such as Cyrex only identify immunological reactions but are blind to adverse food reactions caused by microbial or digestive issues, which makes them somewhat worthless.
The best diagnostic tool to find out whether one reacts badly to a certain food is likely a cumbersome exclusion diet.
Superfoods
Over the years, I have tested many and none did have a significant impact besides stimulating the economy. So far, the only superfood I have found is olive oil, which I consume a lot (normally about 200-300ml per day). Olive oil contains large amounts of mono-unsaturated fatty acids, which everybody seems to do well on from a metabolic perspective. Furthermore, olive oil contains a number of antioxidants.

Thoughts on veganism
One of my friends has been vegan for about six years and has great energy, mood, and health. Another of my friends would like to be vegan for ethical reasons, but every time he tried to go vegan he became depressed a couple of months after transitioning to a vegan diet. He believes that this is due to a deficiency of something that cannot be had through multivitamin supplementation.
Some people seem to tolerate a vegan diet fairly well, whereas others get physical and mental health issues.
The vegan diet contains only meager quantities of a variety of nutrients, including creatine, carnosine, choline, carnitine, coenzyme Q10, taurine, zinc, iron, and vitamin B12. Studies consistently show that vegans have reduced blood levels of many of these. I discuss these nutrients in more detail in the next section on nutrients & supplements.
Some of these are synthesized endogenously to some extent, but the individual capability to do so varies. Speculatively, this is one reason some people fare badly on a vegan diet. Overall, I believe a vegan diet is great for ethical reasons, but not optimal for health reasons (unless one is willing to take a load of supplements – far more than just vitamin B12 and iron). While a mostly plant-based diet seems to be healthy, full-fledged veganism is probably not.

There are some (epidemiological) indicators that a plant-based diet may be associated with longevity. Is this purely due to the healthy user bias? Is this because vegans unconsciously restrict leucine and methionine, two amino acids that activate the mTOR pathway? Is this due to nitrates, vitamins, or antioxidants found in plants? We still do not know though all of these may play a role.
Intermittent fasting
I have experimented with many forms of intermittent fasting. Intermittent fasting is the easiest, the most enjoyable, and the most effective approach to give me dietary freedom, effortlessly low body fat, mental clarity, and simply have me perform at my best. Or at least I once thought so. Well, all it did was lead to disordered eating and damage my body and mind like few other things ever have.
Reportedly, for some individuals intermittent fasting can lead to feeling awesome, sometimes even for prolonged periods of time. For others, not so much. I was in the latter group. We are all different.
I discuss my experience with intermittent fasting in more detail here.
Ketogenic diet
A couple of years ago, I was on variations of a keto-style diet for a little over a year. This wasn’t overly well received by my friends, family, and girlfriend due to the difficulties in eating together. However, my sleep requirements went down by over an hour, which was worth a lot to me. My experience was okay, though, after a couple of months, I started to burn out as I did with intermittent fasting.

On a ketogenic diet, insulin levels are kept extremely low, which results in a rise in blood ketone levels, weight loss, a diminishment of appetite and cravings, stable energy levels, reduced sleep needs, upregulation of autophagy, and a decrease in inflammation. Together, these upsides make ketogenic diets quite useful in the right context.
Dr. Peter Attia claims that a ketogenic diet works especially well for three groups of people:
- ultra-endurance athletes
- type II diabetics
- individuals that cannot afford ups and downs in energy levels (e.g., day traders)
However, applied in the wrong context, a ketogenic diet can also be quite harmful. I share my experience and thoughts on a ketogenic diet in more detail here. I also discuss two drugs that can make adhering to a ketogenic diet easier.
Multi-day fasting
I have done about fifty or so 36–48-hour fasts, about ten or so 5-day fasting-mimicking fasts (eating about 500kcal per day in the form of vegetables and unsweetened peanut butter), and one 9-day water fast.
During my fasts, I supplemented with extended-release potassium (400mg four times per day), salt (3-5g per day), magnesium (600mg per day), and calcium (200mg per day). Interestingly, whenever I consumed a lot of calorie-free sweeteners (mostly in the form of gum and diet Coke), I was kicked out of ketosis and felt awful.
Multi-day fasting has a lot of upsides, and on paper, it is protective against a host of chronic diseases. Multi-day fasts are thought to promote metabolic flexibility, help with metabolic health (insulin resistance, lipid levels, blood pressure, etc.), ramp up autophagy and potentially induce apoptosis of senescent cells and a proliferation of stem cells.

However, for me, it has done more harm than good. For example, it caused a loss of muscle mass, and it screwed up my hormones and metabolism. The major benefits I noticed were a feeling of accomplishment and a build-up of self-discipline. During my fasts, I usually became a productive demon completing about two weeks’ worth of tasks in only five days.
In sum and in my opinion, fasting kills vitality in the long-run and is only net beneficial if one is metabolically unhealthy or overweight. I do not plan on returning to multi-day fasting during the next couple of years, potentially forever.
I share my experience with multi-day fasts in more detail here.
Carnivore diet
Two friends of mine claimed that the carnivore diet helped them with self-diagnosed autoimmune problems. It perhaps did so by removing food allergens, reducing insulin and IGF-1 levels (and therefore reducing mTOR-pathway-associated inflammation), or by bringing about changes in the microbiome due to the starvation of the microbiota in the large intestine.
I like what Dr. Peter Attia has to say about it: “One has to be careful because the cheerleaders are the ones you’re hearing the most. You don’t get to see what the graveyard looks like for all of the people who tried carnivore and didn’t have favorable results.”
Both of my friends have been quite vocal about the carnivore diet as they were starting out, wanting everybody else to try it. Both have quit it quietly.
Thoughts on the microbiome
In my opinion, the microbiome is far less important than what it is currently made out to be. I discuss my thoughts on the current microbiome mania here.
Thoughts on other diet-related topics
Because this article is already awfully long, I share my thoughts on a number of other dietary topics including protein, meats, salt, fiber, dairy, sugar, legumes & grains, and artificial sweeteners here.
My diet in more detail
In the past, I have been experimenting with intermittent fasting, low-carb, paleo, and keto-style diets for multiple years. Nothing else I have done, and I have done a lot, has worsened my vitality as much. It has also wrecked my metabolism, hormonal health, and appetite regulation. The damage took a long time, and pharmaceutical intervention, to recover from.
Hopping on the GLP-1 agonist semaglutide (discussed here) had shown me how much of my day was taken up by thinking about food. Since considerably increasing my caloric intake, I feel much more energetic and alive. After 3 years on the drug, I came off it because I want to gain body mass.
I now follow three loosely held rules to which I aim to adhere about 80% of the time:
- Cutting out most of the processed food and sugar (80/20 principle)
- Eating the highest possible number of calories that does not result in fat gain (which was much higher than what online calculators led me to believe)
- Making sure that my carbohydrate intake is appropriate for my leanness and activity levels
The consistent program that I follow is better than the perfect program that I quit. I believe that if I follow these points, I get a major share of what is maximally attainable through dietary intervention.
Many people treat diet like religion, but, in my opinion, diet is actually not that important if a couple of principles and rules are adhered to. Going from a terrible diet to an okay diet has huge benefits but going from an okay to “perfect” diet (whatever that means) is probably somewhat of a waste of time and energy.
I believe that if I am already on a reasonable diet, dietary intervention is a low-leverage lever to pull, especially compared to sleep and exercise.
On workdays, about 60-80% of my calories consist of Huel shakes. To each shake, I add about 70ml of olive oil to increase fat content and one scoop of whey protein to increase protein content, making each shake about 1200 kcal (about 100g fats, 45g carbs, 55g protein). I am usually drinking 1-2 of these shakes plus a 1-2 normal meals and perhaps a snack.
(Update: I switched out the Huel shakes for Kefir yogurt drinks (500ml) – mostly because the kefir bottles are smaller than the Huel shakes and can more easily fit into my backpack. Furthermore, kefir drinks only contain half the volume compared to Huel, cutting down on the number of times I need to go to the toilet. I also love the taste (though few people I have given them to try do). To each I add 70ml of olive oil and one scoop of whey, making each drink roughly 850 calories. On work days I usually drink 2-3 (mostly 3) per day. I personally like dairy products and react well to them. While a high dairy intake is probably not “optimal” for many reasons, I do not really care because I like it and I love the convenience associated with it. Furthermore, dairy elevates IGF-1 levels. Compared to most people in the health-sphere (“dairy/IGF-1 causes cancer”), I do think that there are more upsides than downsides with slightly higher IGF-1 levels. Ever since embarking on a high-dairy diet, my ApoB levels rose from the 3rd to the 6th percentile – though, for some people dairy might be harsher on their lipid profile due to polymorphisms in the PPAR-transcription factor family.)
The biggest upside of a diet like this (i.e., getting over 50% of my calories from meal replacement drinks (first Huel, now Kefir) is the convenience – it takes me about one minute to prepare. It does not lead to a noticeable increase in blood glucose levels. I never need to worry about hitting my calories, good fats, and protein intake. Furthermore, I never have a post-meal energy slump, and it gives me stable energy for hours. The taste is okay. While my diet is certainly far from “optimal”, I hit my calories, macros and rarely eat junk – the most important points anyway.
On non-work days I am much more flexible and liberal with my diet. However, as said, I believe diet is not as important as it is usually made out to be (given that the diet is already okay-ish) and is overrated compared to sleep, metabolic health, exercise, or hormones.

Related articles
Sources & further information
- Scientific literature: In my opinion, the scientific literature is of little value when it comes to answering questions about diet as most of the available literature is based on epidemiology. Furthermore, there is presumably no other field in which scientific “evidence” contradicts itself so much.
- Scientific article: Mediterranean diet and health status: Active ingredients and pharmacological mechanisms
- Podcast: Peter Attia (The Drive): How Fructose Drives Metabolic Disease
The “top-down” component
I conclude Part I with a note on “psychology”. I like to divide factors that influence my mind into “bottom-up” and “top-down”.
- “Bottom-up” factors are any biochemical changes that influence my mind, including neuropharmaceuticals, sleep, exercise, and hormones. (This entire article is almost exclusively about bottom-up effects, except for perhaps community, purpose, and psychedelics).
- “Top-down” factors are primary mental changes that then influence biochemistry but may also have non-biochemical effects.

In the following paragraphs, I describe my experience with top-down factors and the effects they had on my physiology.
On some days I am tired. If I then do something that excites me, such as having a deep conversation with a friend, it is always striking how this increases my energy and mood. In the same way that a good conversation can have a stimulant-like effect on me for a few hours, so can working on a project I burn for stimulate me for weeks to months. Biochemically, this is presumably mediated in part by a top-down mediated increase in a variety of neurotransmitters.
A few more examples:
- A decade ago, I used to be semi-depressed for about half a year or so because I was reducing myself, my thoughts, and my feelings to molecular biology. Then, simply learning about the concept of emergence was quite powerful in terms of boosting my liveliness. In other words, I boosted my liveliness from “within” the mind.
- The few times I fell in love with someone, I was always amphetamine-like stimulated for a couple of weeks, sometimes months. I was euphoric, needed less sleep, was less hungry, and had more energy. The neurobiochemical cascade of falling in love is characterized by higher levels of oxytocin, glutamate, and dopamine, among other things. Interestingly, falling in love is known to increase cortisol secretion by 40-100%. I am quite sure though that something „deeper“ than hormones and monoamines is also in place in the same way that mania cannot be explained by hormones and monoamines.
- Before meeting my ex-girlfriend, I was in quite a bad place mentally. I was lonely, restless, and my “Urvertrauen” (trust in the Universe that things will be alright) was gone. I then saw somebody I was blown away by. On our first date, I knew that we would be a couple soon. After this single date, my Urvertrauen was restored and all the restlessness, loneliness, and unease, which had been there for months, was gone immediately, as if somebody had flipped a switch in my brain – even though my hormones or monoamines had presumably not changed much. This change in how I felt was holding up for months (as we got together). This may seem “duh” to other people but this was quite eye-opening to my bottom-up-biology centered worldview.
- After one of my ex-girlfriends broke up with me, I was devastated for about six months. In the same way that falling in love with her caused a hypomania-like state, losing her led to a state resembling true biochemical depression. The neurobiology of grief is thought to be characterized by an altered monoamine transmission and a dysregulated neuroendocrine control (hormones), among other things.
- In the past, days before a major exam, I was often super stressed, and many aspects of my mental and biochemical functioning were altered. These included heart rate changes, increased sweating, and even altered gut motility.
A few more non-personal examples:
- The placebo effect is a prime example of a top-down effect. The placebo group in antidepressant studies usually measurably improves in a variety of domains. Similarly, being hopeful or simply believing in something can have measurable physio-biochemical ramifications.
- For many people, unresolved trauma can have massive effects on neurobiology, endocrine function, and physiology – sometimes for years.
- Children that are mistreated or neglected sometimes fail to thrive (to grow properly). This form of “psychosocial dwarfism” can occur even when adequate caloric intake is provided.
- In orangutan tribes (orangutans are somewhat closely related to humans), there is only one alpha male and something about the sheer presence of an alpha male has other male orangutans growth-suppressed (it is thought that his screams play a role). After the alpha male dies, the growth-suppressed young orangutans suddenly go through puberty. This means that puberty was induced from “within the mind”.
In all of these instances, biochemical changes are induced “top-down” (from within the mind) solely due to “information”. It is therefore not too far-fetched to claim that, for example, having a pessimistic or nihilistic mindset can sustainably alter monoamine transmission and hormones, and presumably things that are even “deeper” (e.g., gene expression), negatively (which then in turn favors a nihilistic or angst-ridden mindset).
On the other hand, it has been shown that positive thinking, gratitude, optimism, or “purpose” can have striking effects on neurobiology, endocrine function, and physiology. (This is not to say that biochemical enhancement is not useful in finding purpose, love, or developing an optimistic mindset in the first place.)
Andrew Huberman and Jordan Peterson discuss the influence of “purpose” and “meaning” on dopaminergic neurotransmission here.
Thus far, I heavily relied on biochemical strategies to solve a variety of problems. While it definitely worked, I feel that I know quite little about “mindset” and other “psychological” strategies that help me to feel and perform better. I plan on changing this in the future.
The main point of this entry is basically that vitality can be quite deeply affected by not just changes that are bottom-up (e.g., altering hormones or neurotransmitters trough lifestyle of exogenous molecules) but also by more “psychological” changes (i.e., information), which eventually affect deep material processes within the brain, and presumably also within individual cells. While this may seem “duh” to most people, for me, a biological materialist at heart, this was quite eye-opening to find out about – even though the biological mechanisms are far from being elucidated.
Sources & further information
- Podcast: Andrew Huberman & Jordan Peterson – Neuroscience Meets Psychology
- Website: Wikipedia – Psychosocial short stature
- Opinion article: How to Find Purpose In Life
Part III. Nutrients, Supplements, Blood Tests
Nutrients & supplements
I supplement a lot of stuff. My general supplement framework is to add a low dose of something that is already occurring in my body under natural conditions. My experience and thoughts on herbal supplements are discussed at the end.
- Salt
- Omega 3
- Vitamin D
- Magnesium
- Folate
- Iron
- Selenium
- Vitamins
- Niacin
- TMG
- Creatine
- L-carnitine
- Alpha-lipoic acid
- Beta-alanine
- L-citrulline
- Taurine
- Coenzyme Q10
- N-acetylcysteine
- Glycine
- Phosphatidylcholine
- 5HTP
- Probiotics & prebiotics
The following section may be a little technical – feel free to skip it.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Salt
Because my diet contains few processed foods, my salt intake is quite low. Therefore, I supplement with a 1g sodium chloride tablet in the morning.

For a long time, I thought that restricting salt intake was healthy. However, it may be that most of the health benefits of sodium restriction come from the elimination of processed food. In my opinion, healthy people on a healthy diet are at a greater risk of sodium deficiency than excess.
Omega 3
I supplement with about 2g of EPA/DHA per day. I take it in liquid form because capsules often have unnecessarily high amounts of Vitamin E. To increase bioavailability, I take my fish oil with meals.
Omega 3 fatty acids (EPA/DHA) are important for a lot of different things. They are the building blocks for anti-inflammatory eicosanoids (e.g., resolvins), they act on “master control” transcription factors for metabolism (PPARs), and they are precursors to structural and signaling molecules in the brain.
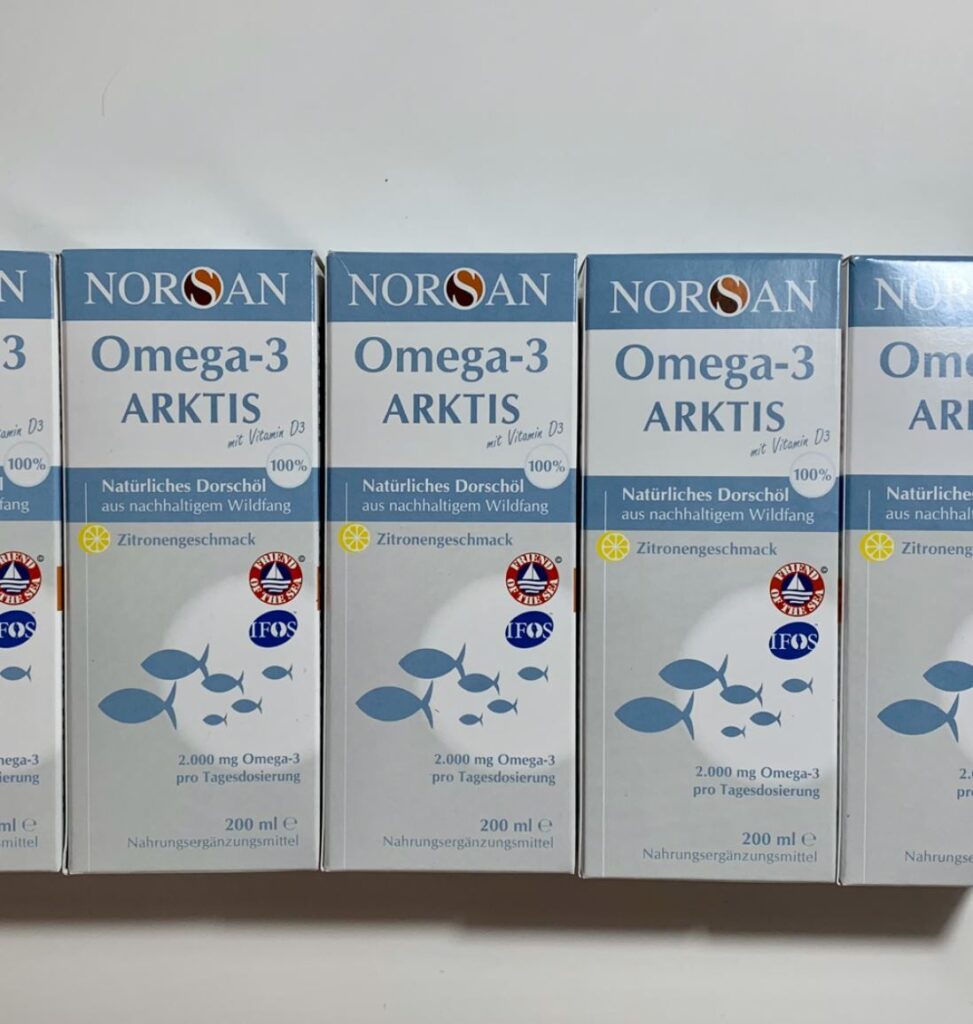
There is evidence that a higher intake may improve metabolic health and lipid markers, lower inflammation, and improve cognition and mood, among other things. Some researchers hypothesize that most people are likely deficient in omega-3 fatty acids by a factor of five or so (based on measurements of phospholipid ratios in the membrane of red blood cells).
Most importantly, epidemiological data hints at the possibility that an increased omega-3 intake may be associated with a reduction in all-cause mortality.
40%-50% of the brain is composed of PUFA. DHA is the main building block and most common in the brain. EPA is less abundant but may have more anti-inflammatory properties compared to DHA. Therefore, elevating O3-fatty acid intake may be somewhat protective against dementia.
Vitamin D
I supplement with 4.000 IU per day, which is likely a dosage that can safely be taken long-term. I titrate my vitamin D intake to a blood level of 40-60ng/dl. Higher levels are not necessarily better and may lead to higher plasma levels of plasma calcium, with potentially deleterious consequences.
Vitamin D is a steroid-like hormone that affects about 5% of the human genome with downstream effects on cognition, mood, immune regulation, and bone metabolism. Just in case, I also supplement with 100mcg vitamin K2, though there seems to be little proper science behind it.
I personally have a couple of single nucleotide polymorphisms associated with lower vitamin D levels. However, does that mean that I need more vitamin D? Unfortunately, blood levels tell me little about what is happening within my cells, and therefore vitamin D blood levels may give an inaccurate picture of cellular action.
In fact, there is a huge range of vitamin D blood levels and it is hard to say whether a vitamin D blood level of 30ng/dl in person A is equivalent to 30ng/dl in person B. All else being equal, if parathyroid hormone (PTH) is high, vitamin D action is (probably) low.
According to Dr. Peter Attia, it is probably best/safest to target a vitamin D level of 40-60ng/dl but not higher than that.
Magnesium
I take 400mg of magnesium citrate or bis-glycinate before bed. I avoid the oxide form as it is poorly absorbed and is mostly useful for helping with constipation.

Due to current harvesting practices, our soils, and consequently a lot of people, are magnesium deficient. Magnesium is needed for hundreds of different enzymes and if magnesium levels are deficient, a lot of cellular processes are not working as intended.
Folate
I take 1mg of L-methyl-folate per day. I take the methyl form because I have a couple of genetic polymorphisms (SNPs) associated with poor performance of the MTHFR pathway. Nonetheless, I do not notice anything whether I take it or not.

Folate deficiency can wreak havoc on monoamine levels and many aspects of cognition and therefore, a psychiatrist I know frequently prescribes L-methylfolate to his patients.
Quick thoughts on the MTHFR gene. A large proportion of people (probably around 50-60% in the Western world) has one of two common mutations in the MTHFR gene. MTHFR codes for an enzyme that is involved in the methylation cycle. It is commonly thought that carriers of the mutated forms should supplement with methylated versions of B vitamins. For example, this is the reason I supplement with L-methyl folate.
In my opinion, the importance of these “mutations” is highly exaggerated. Furthermore, given their prevalence, these “mutations” should be considered wild-type versions. In my opinion, while it may sound cool to claim that one’s depression or ADHD is ultimately caused by a genetic mutation, this most likely does not represent reality. The most worrisome consequence of being a carrier of these kinds of mutations is elevated levels of homocysteine (which wreaks havoc on vascular health).
The only proven longevity supplement
The only supplement I take that is not naturally occurring in my body is astaxanthin, which is the only proven longevity supplement. I discuss my reasoning in more detail here.
Iron
I check my ferritin levels a couple of times per year. Whenever they are low, I supplement with 80mg sustained-release divalent iron per day for a couple of weeks, but I stop before ferritin levels reach about 50-70mcg/L.

Iron is not just important for red blood cell production, but sufficient cellular iron is also important for a lot of other things. High iron levels are associated with increased mortality – however, it is unclear whether that is a consequence or a cause.
Of note, ferritin levels may be falsely elevated if cytokines levels are high. Cytokines stimulate both ferritin synthesis and CRP expression, so one indicator that
cytokines are high is if CRP levels are above 0.5 mg/dl.
Blood tests are discussed in more detail shortly
Selenium
I take 100mcg of selenium per day. Next to being a potent antioxidant, selenium is a component of deiodinase enzymes, which are responsible for converting the prohormone T4 into the active thyroid hormone T3. I discuss thyroid hormones here.

Vitamins
Every couple of days, I take a low dose of a vitamin B complex with a just-in-case mentality. I also take 250mg of vitamin C per day.
I regularly supplement with vitamin D and B12 and monitor my levels through blood tests. Because my vitamin B12 does hardly improve with oral supplementation, I inject 3mg B12 twice per year intramuscularly, which improves serum and storage levels for a long time.

Niacin
I take 250mg of niacin (flush version) a couple of times per week. I would like to take it more often but it seems to screw up my voice for many hours after, presumably due to the laryngeal edema the flush causes.
Niacin is vitamin B3. Niacin is known to reliably elevate intracellular NAD+ levels to a similar extent as the much more expensive supplements NMN or NR – which are mostly a marketing scam because sellers are very aware that the same benefits could be had by niacin.

Furthermore, niacin activates the hydroxycarboxylic acid receptor 2, which causes flushing (good for the skin), prevents lipolysis and therefore lowers blood lipids, which on the one hand leads to rebound ketogenesis (good) but also increases insulin resistance for a couple of hours. Furthermore, HCA 2 receptor activation also has anti-inflammatory effects in a variety of tissues.
I particularly love the flush and I find it to be quite stimulating. For example, when I am tired but I need to work on something, taking 250mg of niacin stimulates me for a couple of hours, presumably due to flushing causing a loss of body heat or due to the elevation in blood ketone levels. Whatever the case, it essentially replaces taking a stimulant. Stimulants are discussed in more detail here.
The major downside of flushing is that my voice gets hoarse and weak for a couple of hours after, presumably due to the flushing-induced laryngeal edema. Of note, a friend got ocular edema from high-dose flush-niacin, so this is something to watch out for. Furthermore, high-dose niacin intake can increase uric acid levels.
Some mental health researchers swear by high-dose niacin but whether there is anything to it is not known.
Tri-methyl-glycine
I take 1g of TMG per day to replete hepatic methyl-groups (which are known to be depleted by niacin), and to reduce homocysteine levels (an autoreactive metabolite thought to speed up the progression of atherosclerosis).

Creatine
For a long time, I did not take creatine because even 1 gram per day of the monohydrate caused me to retain a lot of water and to look like Mrs. Puff. I also felt bloated and had gut issues. I have none of these problems with creatine HCL, of which I take 1 gram per day.
With creatine HCL I do get intracellular water retention (as measured by the scale and judged on muscle fullness) but it does not cause me to hold water subcutaneously – at least not to a noticeable degree. I speculate that subcutaneous water retention is not related to the creatine itself but rather due to the creatine-induced gastrointestinal bloating, which, presumably through vagal afferent nerve fibers, causes an increased hypothalamic release of antidiuretic hormone (ADH), similar to what happens when people have diarrhea. This is pure speculation, however.

The exercise benefits as well as the cognitive benefits of creatine are due to the elevation of cellular creatine-phosphate levels, which aid in ATP regeneration and therefore improve cellular energy generation.
Creatine also seems to have some efficacy in the treatment of depression. It even seems to be able to induce mania in bipolar people, albeit rarely. An ability to induce a manic switch is an indicator that it is doing something in the nervous system.
L-carnitine
I take 500mg of acetyl-L-carnitine per day. I do not take more than this because, in some people, L-carnitine can be metabolized to TMAO, which is thought to increase the risk for cardiovascular disease.

L-carnitine is a mitochondrial fatty acid shuttle. By improving beta-oxidation, it is an antioxidant with potentially nootropic and exercise benefits. L-carnitine is also associated with a reduction in liver enzymes, presumably because of its involvement in fatty-acid oxidation and/or its anti-inflammatory properties.
Alpha-lipoic acid
I take 100mg per day. ALA may be one of the most potent antioxidants out there because it induces the transcription of antioxidant enzymes at the genetic level instead of just being an antioxidant itself. Furthermore, ALA is a metal chelator.
I am still quite unsure about the risk-benefit ratio of antioxidants because in recent years it has become clear that oxidative stress is not merely pathological but ROS leaks serve as signals in many diverse physiological circumstances, such as immune activation and intracellular homeostasis. For now, I keep taking low doses of different antioxidants.
Beta-alanine
I take one gram per day. Beta-alanine is the precursor to carnosine, which protects against exercise-induced lactic acid production (it buffers cells against changes in pH). Beta-alanine is also thought to have anti-glycation and metal-chelation benefits.

Some people believe that beta-alanine is a reasonably powerful anti-aging supplement, though conclusive evidence is lacking. I like the whole-body tingling it causes.
L-citrulline
Sometimes I take 1g of l-citrulline before exercising but most of the time I forget it.

Citrulline converts into L-arginine, which is a precursor to nitric oxide (NO). NO is a vasodilator, and crucial to cardiovascular health. Of note, a lot of the anti-aging benefits from vegetables may come down to their nitrate content.
Taurine
I take 500mg of taurine at night. Taurine is known to increase GABAergic neurotransmission, and therefore may help with deep sleep. Furthermore, taurine is an osmolyte, a metal chelator, and a glycation inhibitor. Whether this is of any practical relevance, I have no idea.

Interestingly, taurine is an essential vitamin for cats, as cats are incapable of synthesizing it by themselves.
Coenzyme Q10
I take 60mg of CoQ10 per day. CoQ10 is an electron shuttle in the electron transport chain. It is also an antioxidant. According to published literature on the subject, it may increase time to exhaustion and anaerobic threshold in both trained and untrained individuals.

It is also frequently added to statin treatment because statins impair CoQ10 synthesis.
N-acetyl cysteine (NAC)
I take 300mg of NAC per day. N-acetyl cysteine is a precursor to L-cysteine, which is a component of glutathione, one of the body’s most important intracellular antioxidants. If taken orally, NAC is a great way to support liver antioxidants.

Furthermore, NAC is thought to “normalize” glutamate signaling and may therefore be useful for states characterized by impulsivity (e.g., anger, anxiety, OCD, or addiction). However, the other side of the coin is that high doses of NAC may lead to emotional blunting. While some emotional blunting may be desirable in states of depression and anxiety, it is not particularly life-enhancing – quite the opposite. Depression is discussed in more detail here.
For me, the selling point of taking NAC was a genetic test. I have a deleterious SNP in a specific N-acetyltransferase, which is associated with lower NAC levels and therefore carries a greater risk of age-related hearing loss. I discuss my other genetic test results in more detail here.
Glycine
I take 5g of glycine at night. I mainly take it because it improves my sleep, which it does in a way I can subjectively feel.

Glycine is an amino acid that serves as a neurotransmitter, acts as a precursor to some other molecules, and regulates the activity of certain enzymes in various metabolic pathways. Glycine plays a special role in methionine metabolism, which is associated with mTOR activity.
Interestingly, glycine passed the Interventions Testing Program (ITP) of the National Institute of Aging, prolonging the lifespan of mice by a tiny but statistically significant amount (4%). However, they put glycine in the chow, which is different than a megadose on an empty stomach, thereby probably having a different safety and effect profile. Paradoxically, glycine is known to activate mTORC1, which should have pro-aging effects.
Phosphatidylcholine (lecithin)
I take 2400mg of phosphatidylcholine per day, which contains about 300mg of choline. Similar to other nutrients found in animal products (such as carnitine, creatine, carnosine, etc.), humans are capable of de novo synthesis but usually endogenous choline synthesis is insufficient to meet “optimal” requirements. Choline is one of these nutrients that a lot of people are probably deficient in.

Choline is a methyl-group donor. It is required for the synthesis of cell membrane lipids including sphingomyelin and phosphatidylcholine, the synthesis of the neurotransmitter acetylcholine (discussed in more detail here), the synthesis of tri-methyl-glycine (discussed previously), the synthesis of S-adenosyl-methionine (discussed shortly), and the synthesis and export of VLDL particles.
A choline deficiency is associated with decreased cognition, depression, atherosclerosis, increased homocysteine levels, and fatty liver disease.
I chose phosphatidylcholine as my choline source because it is well absorbed and because it has a lower risk to be metabolized into TMAO by intestinal bacteria (which increases the risk for atherosclerosis).
Occasionally I take 300mg alpha-GPC, another choline precursor, on days I am particularly tired. Relatedly, I discuss my experience with nicotine here.
5HTP
5HTP is a precursor to serotonin. I do not take 5HTP and if I would, I would take a catecholamine precursor such as L-tyrosine along with it for monoamines to not get out of balance. Monoamines are discussed in more detail here.
Prebiotics and probiotics
Anecdotally, some of my friends benefitted from specific probiotics (e.g., irritable bowel syndrome) whereas others were harmed by them (e.g., indigestion, brain fog, etc). It seems that whether someone benefits from probiotics depends on the probiotic in question and also on the person.
Prebiotics, and particularly probiotics, have always made things worse for me. Nonetheless, during my “gut flora tunnel vision”-time, I did care about my gut health way more than I do now.
Some of the things I did:
- I avoided gut-irritating stuff such as carrageenan, NSAIDs, and alcohol. I also avoided eggs as I seem to react badly to them. Furthermore, I avoided probiotics as, all things considered, they seem to be a net harm for most people.
- I focused on a diet rich in whole foods and fiber.
- I supplemented with psyllium husk (10g/d) to increase bulk, promote bowel movements, and increase the microbial secretion of short-chain fatty acids (SCFA).
- I supplemented with inulin (5g/d) to help with increasing “good” gut bacteria, such as certain species of lactobacilli and bifidobacteria. Acacia fiber is very similar and can be called a “slow-release inulin” and was particularly helpful to adapt to inulin supplementation.
- I ate small amounts of fermented foods every day (e.g., a couple of spoons of sauerkraut). However, it seems that some people tolerate them poorly. For example, a friend of mine reacts badly to them, because, according to him, he gets swamped with histamine, which may be able to cross the gastrointestinal barrier in individuals with increased gastrointestinal permeability (“leaky gut”).
- Twice, I tried to “reset” my gut flora by a taking short course of rifaximin, a gut-targeted broad-spectrum antibiotic.

I believe that the fuzz around the microbiome is one of the greatest shitshows currently going on in the health sphere. I share my thoughts on the microbiome mania in more detail here.
S-adenosyl-methionine (SAM-e)
In the past, I have been taking low doses of SAMe (200mg) for a prolonged period of time. It is the only supplement I have ever tried that has true mood-elevating effects. Unfortunately, recently a study came out suggesting that SAMe may be potentially epigenotoxic, so I stopped.
SAMe is a molecule that serves as a primary methyl donor in several biochemical reactions. These methylation reactions are crucial for the regulation of gene expression, the synthesis of neurotransmitters, and the maintenance of cellular structure and function.

Because SAMe is quite powerful it deserves its special mention. I discuss it in more detail here.
Why I do not use peptides
I discuss my personal experience with peptides and why I am literally scared of using them in more detail here.
My supplement stack
Morning:
- 1g sodium chloride
- 2400mg lecithin
- 500mg L-carnitine
- 1g TMG
- 1 mg L-methyl folate
- 2g creatine HCL
Noon:
- 1g beta-alanine
- 45mcg VitK2
- 100mg alpha-lipoic acid
- 2g EPA/DHA
- 4.000 IU vitamin D
- 250mg VitC
- 60mg CoQ10
Evening:
- 400mg magnesium
- 500mg inositol
- 5g glycine
- 500mg taurine
- 300mg NAC

I am quite sure that some -perhaps even most- of these are a waste. However, it is hard to figure out which ones, and as MD Peter Attia likes to say, at the end of the day, $1 is $1. Speaking of money, all my supplements cost me about 500 Euro per year.
If I only could take 5 supplements, they would be omega-3 fatty acids, magnesium, vitamin D, lecithin, and salt.
I am also quite sure, that compared to diet, exercise, sleep, and hormone optimization, these supplements do laughingly little. I take most of them with a “just-in-case” mentality, and I am equally uncomfortable taking them compared to not taking them. Nonetheless, I have been taking these supplements for about 4-5 years now, and nothing “bad” has happened.
One of the major things I am unsure about is taking three supplements (L-carnitine, betaine, phosphatidylcholine) that potentially convert into TMAO, which is associated with cardiovascular disease.
Reading about various supplements makes it seem that each of them has great benefits for a number of domains. However, everyone who has tried various supplements and is not super prone to the placebo effect can attest to that simply not being the case.
I want to end this section with a quote from an Examine.com newsletter:
“After many years of reviewing supplement research, and publishing peer-reviewed articles on supplements, I can safely tell you: supplements aren’t among the most important parts of a typical health strategy. Some of the most important parts all happen to start with the letter “S”, funny enough, so they’re easy to remember: sleep, stress management, and socializing. These factors, along with emphasizing a diet low in ultra-processed food and getting enough movement each day, should take up a big chunk of your self-improvement efforts. If you’re spending a lot of time and money on supplements, that may be distracting from these big issues that have outsized impacts on health.”
Posting this quote may seem hypocritical from my side, but I nonetheless feel that it is worth sharing.
A note on manufacturers
The supplement market is the wild, wild west. Billions of dollars can be made very cheaply. There is no regulatory oversight that would stop supplement companies from fooling customers in any way possible.
In many cases, the dosage, purity, consistency, quality, presence of byproducts, and bioavailability varies widely. Sometimes the actual amount varies from pill to pill – even within the same batch. Buying from unregulated manufacturers (i.e., supplement companies) is a hit or miss.
Even industry-leading brands like Thorne fail to disclose their CoAs (Certificates of Analysis) from 3rd party testing facilities. Given that independent positive CoAs are a huge advertisement, there is no reason to keep these private unless they either do not do 3rd party testing or worse, they do but frequently fail.
I personally only buy from Now Foods, Jarrow, Life Extension, and a couple of European brands.
Why I avoid herbal supplements
I experimented with a variety of herbal supplements (e.g., rhodiola, ashwagandha), but I decided to ditch them altogether. I discuss my experience and thoughts on herbal supplements in more detail here.
Sources and further information
- Website: Wikipedia – Articles on each of the individual supplements
- Website: Examine.com
- YouTube: The Attia Rule of Health
Blood tests
Four times per year, I do a blood test and monitor the following parameters, ready to intervene accordingly.

I link to sections where I discuss these markers in more detail.
- Hematology profile
- ALT, AST (GOT, GTP)
- Uric acid
- Creatinine
- HBA1C
- Triglycerides, HDL, ApoB
- CRP, fibrinogen
- Ferritin
- Vitamin B12, vitamin D, folic acid
- TSH, fT3, fT4
- LH, FSH, total testosterone, SHBG, E2
- DHEA-S
- IGF-1
- Leptin
Every or every other year I test for:
- Lp(a)
- Homocysteine
- Cystatin C
- CMV antibodies
- A couple of tumor markers
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Two to three times per year I wear a continuous glucose monitor (CGM) to reevaluate my diet and metabolic health. I also performed a number of genetic tests, which gave me a couple of interesting and actionable insights. I discuss the results and practical takeaways of these tests in more detail here.
Sources & further information
- Podcast: Peter Attia – What lab tests can (and cannot) inform us about our overall objective of longevity
- Scientific article: Continuous Glucose Monitoring: A Review of Recent Studies Demonstrating Improved Glycemic Outcomes
- Opinion article: Sergei Faguet – Hundreds of biomarkers I test in pursuit of focus, health, energy, confidence and happiness.
Part IV: Hormones
I find that life is much easier and much more enjoyable if I have great energy levels, mood, and health most of the time. In fact, whatever I want in life, great vitality is perhaps the most important requirement to get me there.
As it turns out, my vitality is closely dependent on my hormonal balance. If even one of my major hormones is off, my vitality takes a severe hit, and no lifestyle intervention, supplement, or drug can remedy that.
Conversely, I was more vital, energetic, and emotional during puberty, a time during which most of my major hormones were at their peak.

Many of the major hormones affect every bodily system because they modulate cellular gene expression directly – the deepest and most powerful layer of intervention.
My experiments and experiences with hormone replacement lead me to believe that a sizeable subset of people that have to rely on stimulants to function and be productive may simply have low levels of testosterone, cortisol, thyroid hormones, leptin, or a combination of these.
Some general stuff about hormones
Life consists of cells. Cells are biological machines emerging from the laws of chemistry and physics and just do what they are programmed to. The blueprint for this program is written in the form of the genetic code.

A multicellular organism relies on the different functions carried out by its many different specialized cells and each cell contributes to and benefits from homeostasis, whose ultimate point is survival and reproduction of the organism. For the coordinated function of these many different cells, systemic coordination is necessary.
Multicellular organisms evolved signaling molecules to coordinate the activity and behavior of the different cells separated by a distance. Next to local small-scale coordination via paracrine mediators, there are certain signaling molecules that are used for large-scale coordination of many different cells, tissues, and organs at the same time. These systemic signaling molecules are called hormones.
Some of the major hormones, including steroid hormones (e.g., cortisol, estradiol, testosterone), thyroid hormones, and IGF-1 act on pretty much every cell of the body at the same time. By acting on the blueprint written in the form of the genetic code, these hormones instruct cells on a body-wide level how they should behave.
For example, insulin signals to store nutrients, thyroid hormones determine the metabolic rate, sex hormones instruct the organism to get ready for reproduction, IGF1 induces growth and repair, cortisol instructs cells to prepare for stress, etc.
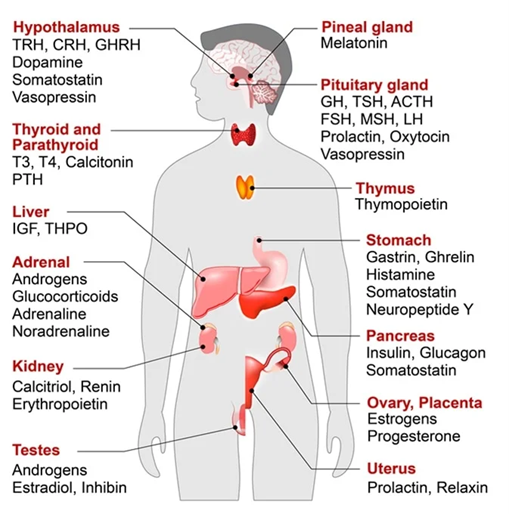
Many of the major hormones achieve this systemic coordination by directly affecting gene expression (among other things) and are therefore among the major determinants of what programs -and to what extent- are running in any given cell at any given point in time.
With very few exceptions, almost every single cell in the human body has millions of receptors for all of the major hypothalamic hormones (sex hormones, stress hormones, growth hormone, thyroid hormones).
Each of them unlocks a specific portion of the genetic code, depending on what part of the code is accessible, which differs between tissues. This is what makes hormones uniquely powerful – far more powerful than a pharmaceutical drug merely affecting a single target.

Each of the major hormones affects each single cell in multiple ways.
- Firstly, as explained above, many hormones have direct genomic effects which alter the expression of the genetic code, sometimes in major ways. For example, testosterone causes the expression of hundreds of genes that have the androgen response element in their promoter region. The expressed proteins then alter cellular function in testosterone-specific ways, such as hypertrophy in muscle cells, maturation in sperm cells, or an increase in activity of dopamine-producing neurons.
- Secondly, hormones have indirect effects because each hormone affects many other hormones and mediators. For example, testosterone affects levels of cortisol, insulin, leptin, oxytocin, and IGF-1, which each then have effects on their own.
- Thirdly, hormones affect energy levels, mood, and health and therefore have a major influence on behavior, which then affects the lifestyle choices people make, which then affects the whole body in a number of ways. For example, testosterone increases energy levels, motivation, and stimulates musculoskeletal changes, which then affect the desire and ability to exercise.
As may be evident by now, if one of the major hormones is off, this will have major effects on the whole organism, ranging from genome, cell, tissue, organ, physiology, behavior, and life situation. Conversely, hormone therapy is perhaps among the most holistic therapies currently available – holistic in the sense of affecting all aspects of the body and mind.
While the mechanism of action of most pharmaceutical drugs is usually high upstream in the signaling hierarchy, many hormones act at the most downstream level possible (gene expression) affecting the whole organism from deep within. Each of the major hormones modulates every bodily system, having powerful effects on the cardiovascular system, immune system, musculoskeletal system, liver, kidneys, brain, etc.
In my opinion, using these natural molecules my body had been adapted to for millions of years is more “natural” and more effective than the current medical practice of sick care (instead of health care) to prescribe a cocktail of different drugs to patch up all the individual symptoms, complaints, and every abnormal physical or laboratory finding separately.
For example, hypothyroidism is associated with fatigue, depression, weight gain, and dyslipidemia. Often, these symptoms are patched up individually with caffeine, antidepressants, metabolic drugs, and lipid-lowering agents.
Why are hormones underused?
Unfortunately, hormones are something doctors rarely properly look at, and hormone replacement therapy is rarely used by most doctors. In fact, many doctors are scared of it. In my experience, most doctors would rather prescribe a cocktail of unnatural drugs instead of the necessary bio-identical molecules. I suspect that this is mostly industry-driven.
Speculatively, hormones are widely neglected by mainstream medicine in part because the evidence for these natural molecules is quite poor. However, absence of evidence is not evidence of absence. The medical system is a huge industry and as is the case with other industries, it depends on revenue generation (“follow the money”).
Most revenue is made from patents. However, hormones are natural molecules, which nobody is allowed to patent. Therefore, since not much money can be made from hormones, they do not have as much evidence behind them as pharmaceutical drugs, given that a lot of evidence generation is funded because of financial incentives.
The evidence-generation process is a revenue-generation process, distorting medical science so much that many physicians have unfounded confidence in unnatural drugs while remaining ignorant and fearful of natural hormones.
Even though not (yet?) widespread, the use of hormone therapy is no secret, and many doctors around the world have recognized their unparalleled power. The focus of these doctors is often on prevention and longevity, trying to keep the patients healthy and functional for as long as possible instead of being financially incentivized by sickness.
Many of these doctors use hormones extensively and have been doing so for decades in thousands of patients. They often balance multiple hormones simultaneously using small physiological dosages. There certainly are risks (as there are with any other therapy) but if doses are physiological, hormones properly balanced with each other, and the proper delivery route used, the risk is much smaller than what conventional medical “wisdom” leads people (and doctors) to believe.
For a long time, many of these doctors have practiced in the background, largely outside the established medical system, and predominantly served the rich and powerful, though it seems that times are changing.
Hopefully, proper hormone replacement will be more widely accessible in the future beyond the domains of “alternative”, “functional”, “complementary”, or anti-aging medicine.
Unfortunately, many people do not like hormones because they prefer “natural” treatment instead. They would rather ingest truckloads of unnatural herbal supplements than administer the natural hormones our physiologies evolved with for millions of years.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Thyroid hormones
Thyroid hormones’s primary role is to increase the metabolic rate of every cell in the body. In simple terms, thyroid hormones make everything faster. For example, this includes the rate at which nutrients are metabolized, neurons communicate, hairs grow, or wounds heal. In addition to increasing the metabolic rate of every cell, thyroid hormones also increase blood circulation, which itself also promotes healthy joints, tendons, skin, hair, and nails.
Thyroid hormone deficiency can produce a hypometabolic syndrome that manifests as depression, fatigue, slowness, brain fog, weight gain, or poor circulation.
It is no coincidence that thyroid hormones are one of the most studied augmentation agents in the treatment of depression. Thyroid hormones stimulate monoaminergic neurotransmitter systems (serotonin, dopamine, noradrenaline) and therefore improve energy, mood, and motivation.
If thyroid hormones improve, antidepressants and stimulants (including coffee) are much more effective and sometimes dosages need to be reduced, or can be phased out completely. Even in non-depressed people, supplemental thyroid hormones tend to improve mood and make the mind “quicker”.
(Of note, in general, many hormones do have potent effects on monoamine transmitter systems. However, monoamines can be high even if hormones are low, and monoamines can be low, even if hormones are high.)
Personal experience
A couple of years ago, I found out that my thyroid hormones are at the lower end of the reference range. After lifestyle interventions did not help (presumably because I was already at my healthy baseline), I decided to take them despite no proven deficiency from a TSH-based reference frame. I do not fully replace my endogenous production but only “supplement” with them.
I had been taking low doses of thyroid hormones for about six years and supplementing with thyroid hormones, in particular a low dose of T3, improved many aspects of my general health, energy levels, sleep, and life enjoyment. I could also work for longer and with more stable energy.
Whenever I stopped taking them, I felt more tired after waking up, my mood and general sense of well-being took a hit, and I needed to drink coffee or take other stimulants to maintain a similar level of functionality, my sleep duration increased, energy levels decreased, and I was cold for a couple of weeks. I also got more infections (which I rarely get).
After a few weeks, things seemed to gradually get better, though, all things considered, I found that, for me, life was a little bit easier and better if I supplemented with low doses of thyroid hormones.
I recently stopped taking them because the addition of metreleptin to my regimen boosted my thyroid hormones from the low-normal to the high-normal range and I felt that the additional T3 dehydrated me and made me a tad more restless. Time will tell whether I go back to thyroid hormones or not.

Signs & symptoms of low thyroid hormones
- needing a lot of sleep
- being tired in the morning after waking up
- getting easily tired at rest
- over-reliance on caffeine
- puffy & pale face (especially in the morning)
- a lowish heart rate
- an inability to lose weight
- having low energy levels
- dry skin & hair & nails
- poor wound healing
- frequent infections
- cold hands and feet
- poor concentration
- slowness in thought
- brain fog
Diagnostics
When it comes to determining hormone function, a blood test is not enough. Just as important are signs & symptoms (and some doctors claim, perhaps rightfully, that signs & symptoms matter a little more than lab values when it comes to diagnosing hormone deficiencies).
- Blood test: TSH, fT3, fT4
- Vital signs: low body temperature, low heart rate, a small difference between systolic and diastolic blood pressure
- Presences of symptoms (see above)
Intervention that worked for me and friends
- Thyroid replacement therapy: Desiccated thyroid or T4/T3 combination therapy – the T3 needs to be taken at least twice per day, ideally thrice. Ideal doses and regimens need some trial & error.
- Avoid: eating too many cruciferous vegetables as they contain goitrogens; only looking at lab values for diagnosis or monitoring treatment
Sources & further information
- Opinion article: Dr. Linder – Thyroid hormone
- Website: Wikipedia – Thyroid hormones
- Scientific article: The Link between Thyroid Function and Depression
Testosterone
High levels of testosterone promote energy, drive, ambition, assertiveness, self-confidence, and purpose. Furthermore, high levels of testosterone promote status-seeking (e.g., through buying expensive cars or clothing). Some of this comes down to the way testosterone increases dopamine signaling.
However, testosterone receptors are widely expressed in the central nervous system and testosterone has effects on many brain sites, particularly in “emotional” centers of the brain. Testosterone also affects cognition in poorly understood ways. For example, testosterone improves spatial thinking and women who excel at mathematics on average have higher T-levels.
Of note, it is hard to say which of these effects are caused by testosterone itself, and which are caused by its conversion to DHT or estradiol. For example, if the aromatization to estradiol is blocked the “testosterone”-mediated increase in aggression and libido declines.
Outside the brain, testosterone has a lot of effects on pretty much every bodily tissue, which is the case for many other steroid hormones as well. For example, testosterone strengthens muscles, tendons, and bones. DHT, the primary metabolite, stimulates the expression of the typical “male” phenotype and affects the growth of the larynx, penis, hair, and prostate.
Personal experience
In my early twenties, I dieted down to very low levels of body fat, and my testosterone levels tanked. I jumped on the TRT bandwagon and replaced my testosterone levels for about two to three years. During this time, I experimented with all kinds of combinations of testosterone cypionate, HCG, FSH, and aromatase inhibitors, but the more I tried to mess with it, the worse I felt. Eventually, I settled on the simplest option: testosterone-only (100mg per week) plus a low dose of HcG (125 IU twice per week).

In retrospect, my experience with TRT was quite underwhelming. There was quite a large placebo effect associated with it as I believed that a lot of my problems with my energy, mood, health, and physique could be solved with testosterone replacement – which was simply not true.
Initially, there was a honeymoon period that lasted for a couple of weeks. After that, I have not noticed much of a benefit other than an uptick in drive and an easier time to build muscle.
It did help my physique though. The difference between left and right is roughly 10kg of lean tissue. On the left, my testosterone was borderline low and I have not yet started going to the gym. On the right, my testosterone was at the top of the reference range plus two years of dedicated training (1 hour of gym three times per week). For a picture of me 2 years after TRT with just dedicated training click here and scroll down to the section on “body fat”.

The major thing I noticed was that I needed less sleep, and I was often fine with just sleeping 6-7 hours, an effect I also experience after two weeks plus of semen retention (which interestingly does not affect my testosterone levels but presumably affects ancient neural circuitry upstream of sex hormone signaling).
Another thing I noticed was that testosterone visibly aged me. After a year on TRT, others have commented that my face seems to have grown older by multiple years. This transition from boyish to manly (which is not necessarily bad) may be in part explained by a redistribution of facial fat but it may also be in part because high levels of androgens drive the aging process.
To some extent, testosterone is like a peacock tail. High levels of testosterone help with signaling “good genes” but at the expense of longevity. Testosterone’s effect on longevity is u-shaped and high levels of androgens are quite bad for every organ system other than the musculoskeletal system and perhaps insulin sensitivity.
Surprisingly, coming off was much easier than expected. I simply stopped injections. I lost a bunch of water weight and my face looked overall much better. After 1 month I was back to my baseline, which is in the 600-700 ng/dl range. Some people have issues with coming off and recovering their natural levels, particularly if they have been using higher doses (e.g., for bodybuilding purposes). Fortunately, I was not one of them.
Thoughts on current trends
Recently, more and more people seem to self-experiment with testosterone. The online landscape paints a picture that everything is explained (and fixed) by the panacea testosterone. From mental health issues, to (lack of) gains at the gym, to motivation and procrastination.
Thus, thousands flock to “TRT clinics”. These clinics are prescription writing factories that will find excuses to give TRT to almost everyone. They make claims that the normal ranges are wrong and the only correct result is to be at the top of, or above, the reference range. They start people on insane beginning doses like 250mg/week because it gives them a rush to feel like it’s “working”.
Spoiler alert: A lot of people are in for a rough awakening…and a prematurely aged body.
Signs & symptoms of low testosterone
- constant low-level background fatigue
- low sex drive
- inability to build muscle
- easily fatigued during exercise
- lack of drive and motivation
- little zest for life
- poor self-confidence
- anxiety and depression
- being skinny fat
- a lot of fat over the triceps area
Diagnostics
- Blood test:
- Minimal: total T, SHBG
- Extensive: total T, SHBG, free T, E2, LH, FSH
- Signs & symptoms
Interventions that worked for me and friends
- Body fat & dieting: In my opinion, the number one overlooked reason for low testosterone is not stress, sleep deprivation, or micronutrient deficiency but caloric restriction or having too little body fat (or chronic dieting). The HPTA axis is quite sensitive to energy balance, particularly leptin levels (discussed shortly), which makes evolutionary sense. Conversely, having too much body fat also lowers testosterone levels, as adipose tissue expresses aromatase, which aromatizes testosterone into estradiol (E2), which then exerts powerful negative feedback on the HPTA axis.
- Dosage & regimen: A decent starting dose is 100mg testosterone cypionate per week split into at least three weekly subcutaneous injections (ideally, daily injections). While I was on TRT I used a low dose of HCG (125IU twice weekly) to preserve fertility and testicular size, however, it seems that daily administration is superior (e.g., 50 IU HCG per day). I only ever used insulin syringes and injected into my upper glute area.
- A note on estradiol: One friend, who is a little overweight, is a high-aromatizer. He uses a low dose of the aromatase inhibitor (AI) anastrozole to keep estrogen levels in check (0.1mg twice per week). In my opinion, the vast majority of non-obese people using physiological doses of T do not need an AI, and in fact, may do net harm by adding one. Estradiol is important for many things, from energy levels, mood, libido, cognitive function, and joint and bone and brain health.
- A note on females: Testosterone is very important for women. In fact, molecule per molecule, there is about 10 times more testosterone in women than estradiol. Unfortunately, testosterone is rarely replaced in females, which is a problem for women who take oral contraceptives or women on postmenopausal hormone replacement therapy, both of which have a large shift in their estradiol to testosterone ratio. Therefore, a gynecologist friend gives either DHEA or low doses of testosterone in addition to HRT.
- Avoid: racemic clomiphene (enclomiphene is okay, though very hard to get hold of), most TRT “clinics”, shady over-the-counter testosterone boosters, 19-nor-steroids (which are very suppressive)
Update on TRT
I am back on TRT, though on a modified protocol that gives me the best of both worlds. Article here: My TRT Lite Protocol
Sources & further information
- Podcast: Peter Attia & Andrew Huberman: Discussion on TRT
- Video: More Plates More Dates: What It Feels Like to Be On Testosterone
- Website: Reddit – r/Testosterone
Cortisol
Cortisol is a very misunderstood hormone. Cortisol is the most motivating and stimulating hormone. Cortisol gives energy, vitality, and “punch”. Cortisol clarifies thinking, sharpens concentration, and improves cognition & memory, giving a “clear” head and a sharp mind. Furthermore, cortisol increases the availability of plasma nutrients and regulates the immune system. All of this makes physiological and evolutionary sense in times of stress and danger.
The right level of cortisol is vital for performance and well-being, and from personal experience, I can say that too little makes life miserable.
Cortisol boosts the release of a variety of neurotransmitters, first and foremost dopamine. Furthermore, cortisol potentiates intracellular dopamine signal transduction. It also upregulates dopamine receptors. For example, after removal of adrenal glands, D1 receptor expression falls by about 40%. Furthermore, very high levels of glucocorticoids can even lead to mania and psychosis (”steroid psychosis”).
Conversely, low levels of cortisol lead to little motivation, anergic depression, and abysmal energy levels. In fact, low cortisol is a surprisingly common but somewhat underappreciated cause of low energy levels and brain fog. Thyroid hormones regulate the “idle state” while adrenal hormones are the “gas pedal”. Both are needed for good energy.
Anecdotally, there are whole underground communities of people who have “got their life” back by implementing low-dose cortisol replacement regimens. Reportedly, some people have been taking supplemental cortisol for many years without (major) issues – though they may artificially accelerate their rate of aging and other degenerative conditions.
Of note, people in the military and other high-energy jobs often have SNPs that are associated with hypercortisolism. These people overproduce cortisol, have a lot of energy, can pull all-nighters easily, and age quickly. I discuss the effect of cortisol on aging in more detail here.
Personal experience
A couple of years ago, I had what some people would call “adrenal” fatigue (better term: HPA-axis dysfunction as it has little to do with the adrenals but everything with hypothalamic function) due to intermittent fasting and undereating.
At my worst, I felt like absolute crap. I needed to exercise vigorously every day in order to feel and function well.
Low doses of cortisone acetate were a godsend.
For a couple of months, I used low doses of hydrocortisone, which helped me out quite a bit. Because I kept doses low, I have not noticed any negative effects on my metabolic health or other aspects. After having recovered, the effects of HC had diminished to the point of being negligible. In fact, if I now take HC I barely feel anything whereas before even small doses were quite stimulating.
I discuss my experience with hydrocortisone (pharmaceutical cortisol) in more detail here.

Signs & symptoms of low cortisol
- abysmal energy levels
- dark under-eye circles
- brain fog
- difficulty waking up
- exhaustion at night
- over-reliance on caffeine
- low blood pressure
- dizziness upon standing up
- sugar & salt cravings
- low body temperature
- difficulty adjusting to changes in ambient temperature (especially heat intolerance)
- scanty perspiration
Diagnostics
- Diagnosing low cortisol is hard. Blood tests, urine tests, or saliva tests are only moderately useful.
- Signs & symptoms (see above)
- Trial-dose of hydrocortisone
Intervention that worked for me and friends
- Rhodiola or ashwagandha for light „adrenal fatigue” (i.e., HPA-axis dysfunction)
- Licorice root (inhibitor of HSD-II enzyme): HSD-II converts cortisol to the inactive cortisone. Even though effective, it is presumably unsafe. When I was taking it, my aldosterone levels were unmeasurable and my 24-hour urinary cortisol profile was drastically elevated, possibly exposing my kidneys to large glucocorticoid loads.
- Lifestyle: stress reduction, sunlight & bright light therapy (especially in the morning), eating enough calories
- Falling in love: Individuals who have recently fallen in love show a drastic increase in cortisol secretion (about 40%) for up to 6 months.
- Specific antidepressants: bupropion, vortioxetine, moclobemide
- Cortisol replacement therapy: However, no dose of cortisol is safe to take long-term. I discuss my experience with cortisol replacement therapy in more detail here.
- Avoid: intermittent fasting, ketogenic diets, caffeine, expensive “adrenal fatigue” supplements
“Adrenal” fatigue
Adrenal fatigue (HPA-axis dysfunction) has many similarities with atypical depression. For example, both have a blunted HPA axis, chronic low mood, fatigue, sleeping in, overeating, laying around all day, and being overly sensitive. And both will improve if hydrocortisone is given. What “label” someone will be diagnosed with depends in part on what kind of specialist people see (whether a naturopath or a psychiatrist). I discuss atypical depression in more detail here.
Sources & further information
- Opinion article: Dr. Linder – Cortisol
- Scientific article: Endocrine Aspects of Burnout
- Scientific article: A Review of Hypothalamic-Pituitary-Adrenal Axis Function in Chronic Fatigue Syndrome
Leptin
Leptin is a master control hormone that regulates long-term energy homeostasis. Leptin is not just a “satiety hormone” as many people wrongly assume, but leptin’s main role is to act as a “starvation signal” when leptin levels are low. Leptin can be considered the body’s “fat report”. It is secreted by adipose cells depending on how “full” these cells are.
We are the only primates that have conspicuous fat deposits year-round, particularly females (e.g., buttocks, breasts). And when these fat deposits run low, our bodies evolved to shut down many physiological and mental processes. The signal for how “full” these fat deposits are is mediated by leptin. Therefore, leptin can be considered the body’s “fat report” as it is secreted by adipose cells in proportion to how “full” these cells are.
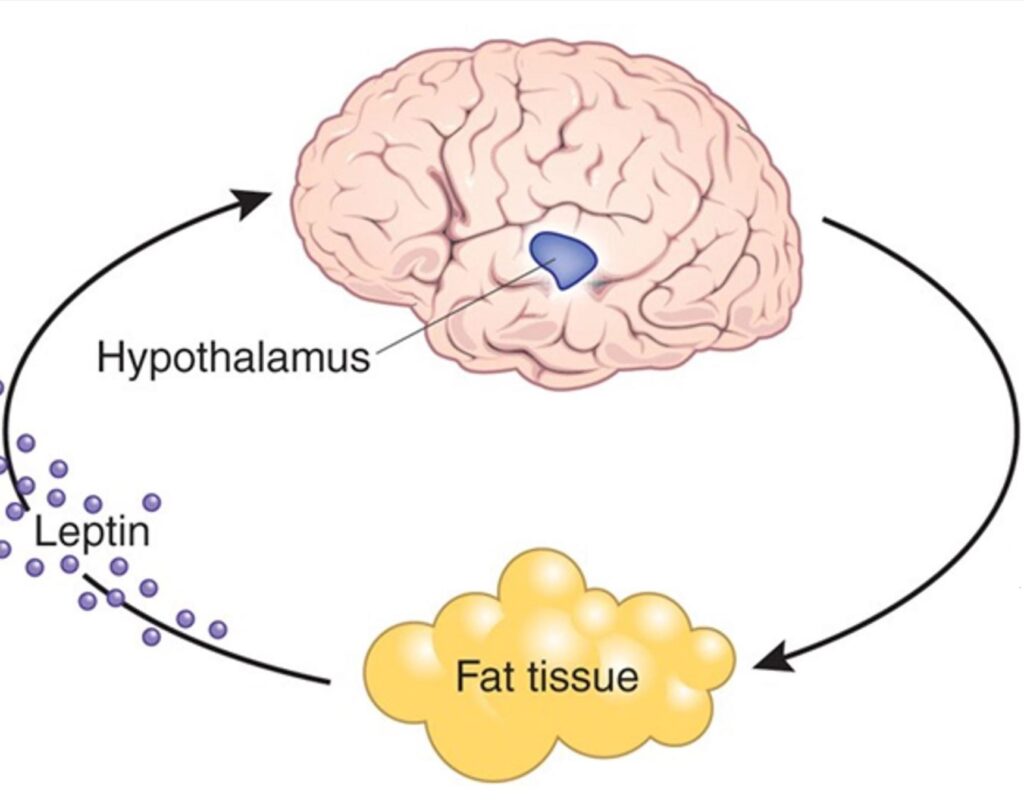
When leptin levels are adequate, this is a “go-ahead” signal for the animal to spend its energy in pursuit of other things besides acquiring food. If body fat levels fall below a certain threshold, leptin levels tank.
When levels get low, all aspects of the organism are driven toward the maintenance of sufficient fat stores for survival. This includes a shutting down of endocrine systems, reproduction, sympathetic nervous system activity, and non-food-related interests. At the same time, appetite, foraging behaviors, and a mental preoccupation with food are all ramped up.
It makes little difference whether leptin levels are “normal” or “high”, but it makes a huge difference if leptin levels fall below a specific threshold, progressively adapting the organism to starvation the lower leptin levels get.

Leptin is flying under the radar and I have never encountered a doctor who looks at leptin levels – not even endocrinologists or other hormone specialists. In my opinion, some unsolved problems with energy levels and hormone problems may be due to undiagnosed hypoleptinemia. Many try testosterone and thyroid replacement but still suffer from some symptoms of hypogonadism or hypothyroidism. Even if said hormones are normalized artificially, many of the symptoms remain if leptin levels are low.
Personal experience
Energy levels have a major say in my charisma, wit, how much fun I am to be around, mindfulness, cognition, productivity, and life enjoyment. But without enough leptin, my energy levels are aweful – regardless of the levels of other hormones.
As mentioned already, a few years ago I dieted down to very low levels of body fat, which I stupidly maintained for quite a long time. I was always lethargic, and it felt like somebody had pulled out my batteries. I also had problems with thermoregulation, my mood and libido were low, and simply moving around felt like an onerous task.
Furthermore, despite the lethargy, I was also quite restless, driven, and my mind was racing all of the time. I was plagued by an inability to sit still and had an irresistible urge to always be productive (presumably a proxy for “foraging behaviors”). I needed to exercise vigorously only to feel normal. I also became socially anhedonic and wanted to be left alone. A lot of my mental brainpower was taken up by food.
I started to replace other hormones, though this only partially helped. This was long before I knew much about leptin.
Recovery took a lot of time, a GLP-1 agonist, and some time on metreleptin (the only currently available leptin analog) to get fully back to normal, presumably because many parts of my brain trophically and epigenetically adapted to “starvation mode” and it took some time, and exposure to high leptin levels, for them to reverse back to “normal mode”.
At the time, my leptin levels were below 1 ng/ml (hypoleptinemia). While this may sound cliché, a couple of hours after my first injection it seemed like somebody had turned the lights back on. I felt a surge in energy levels, my mood became much better, my hunger levels declined, and I was in a distinct state of “presence”.
Before starting metreleptin, I experienced hunger every few hours, even while taking semaglutide (as semaglutide cant exert its effects well if leptin levels are low – as explained in more detail in my article on semaglutide). However, from the first day of using metreleptin, my post-meal fullness improved significantly – I was able to eat and then stay satisfied for many hours.
Furthermore, my dreams became ultra vivid (particularly during the first week), my sleep duration increased, and I felt deeply rested in the morning after waking up, something I had not done for a long time.
I was surprised by the rapidity of the effects, which were in fact immediate.
Interestingly, over the next couple of months, I needed to reduce the dosage by over 50% as the effect of metreleptin seemed to get stronger over time (i.e., I lost nearly all of my appetite and nothing seemed appealing), presumably reflecting trophic changes in the central nervous system. Over the next couple of months, I titrated my leptin levels in a way that would match the leptin levels of a male with 15-20% body fat.
On the physical side, the only thing I noticed was some fat redistribution. Despite not having lost body fat (I actively tried not to by elevating my caloric intake to well above 3000kcal/day), fat redistributed from the facial & trunk regions to my extremities, something that is both metabolically and aesthetically pleasing.
Adipose tissue specifically in my face decreased to the point where many of my friends & family commented on it, particularly my jawline became more pronounced though my cheeks started to look a little gaunt, which caused me to lower my leptin dosage a second time. Metreleptin-induced loss of facial fat is also reported in the medical literature. Overall, my face became significantly more attractive (as judged by female friends).
Replacing leptin essentially lowered my “fat setpoint”, allowing for maintaining very low body fat levels without suffering from lethargy, ravenous hunger, hormone deficiencies, and other starvation-related adaptations, which would obviously be of immense value to the modeling, acting, fitness, and bodybuilding industry.
While procuring the drug was a hassle, it was one of the most interesting and fruitful experiments I had ever done. I may write a more detailed article about my experience with metreleptin at some point in the future as this is something that, to my knowledge, nobody has done (or at least written about) before. To get notified when it is available, sign up for my newsletter.
Symptoms
- hormone imbalances
- low energy levels
- low sex drive
- ravenous appetite
- reactive hypoglycemia
- restlessness
- low sympathetic nervous system activity (e.g., low blood pressure, low heart rate, low body temperature, fatigue)
- persistent symptoms of multiple hormone deficiencies that do not adequately improve with hormone replacement therapy
Diagnostics
- Blood test: leptin
Interventions that worked for me and friends
- Metreleptin: The only currently available leptin analog. Mibavademab, a leptin receptor agonizing antibody, is currently in clinical trials though it is uncertain whether brain sites beyond the circumventricular organs are reached.
- Gaining body fat: Body fat levels are the major determinant of leptin levels. At low body fat levels, leptin levels are low. However, high body fat levels are often accompanied by leptin resistance. Most males feel and function best between 13-18% body fat.
- Semaglutide: Semaglutide is a known “leptin sensitizer”, which means that leptin signaling is stronger. Among other things, GLP-1 agonists are thought to increase the expression of leptin receptors on the order of 40-70% but presumably also enhance intracellular leptin signal transduction.
- Increasing caloric intake: It seems that caloric intake has an effect on leptin levels independent of body fat levels. Furthermore, it seems that a high caloric intake has a leptin-sensitizing effect in the hypothalamus, regardless of body fat levels.
- Increasing carbohydrate consumption: Insulin potentiates leptin synthesis.
- Avoid: ketogenic diets, intermittent fasting, multi-day fasting, dieting
Leptin vs. ghrelin?
There is a widespread misconception that leptin is the antagonist of ghrelin. This misconception implies that leptin and ghrelin play in the same league of importance. Nothing could be further from the truth.
Leptin is one of the few master control hormones, whereas ghrelin serves a few highly specific and to some degree expendable minor functions, exerting its effects on measly G-protein-coupled receptors. Leptin, on the other hand, exerts its effects via a special cytokine receptor, directly linked to widespread and major alterations in gene expression through STAT3 activation.

“I can maintain sub 10% body fat with no issues”
The human body evolved a mechanism that it stops working properly if adipose tissue reserves are too low, presumably for survival-related reasons. However, purely from a functional perspective, there is little reason to assume that humans need to carry more fat than the closely-related chimpanzees.

Even though carrying a decent amount adipose tissue is not needed from a functional perspective, the human body nonetheless evolved to “shut down” when adipose tissue is lacking by way of gradients in leptin signaling.
Every one of us has a different “leptin threshold” level and also a different level of leptin synthesis for a given amount of body fat. Furthermore, individuals differ in terms of leptin sensitivity. Consequently, some people can naturally stay at very low levels of body fat without adverse effects, whereas for others body fat needs to be much higher.
There are a couple of people who claim that they can maintain a sub 10% body fat “just fine”. I suspect that the vast majority of these people are either purposefully lying, have little self-awareness, or are so much used to their state that they have simply forgotten what being in “normal non-starvation mode” feels like.
Obviously, there are genetic differences in leptin secretion per fat mass and/or leptin receptor signaling and some people can truly stay at very low body-fat levels without suffering from starvation-related adaptations – but the vast majority of people cannot.
To test this, if somebody can truly maintain a sub-10 % body fat level “just fine” (or sub-18 % for females), he would not feel anything from metreleptin administration at a dose sufficient to mimic 20% body fat.
Unfortunately, many people do not really recover after dieting down to a body fat level too low (e.g. cold intolerance, anhedonia, loss of libido, lethargy) — online there are many anecdotes of people that seem to have permanently screwed themselves by dieting down too low. Even more unfortunate, leptin agonists (which are next to impossible to get hold of) are perhaps the only thing that can truly reverse these changes without a significant amount of fat gain.
Sources & further reading
- Scientific study: Short-term metreleptin treatment of patients with anorexia nervosa: rapid on-set of beneficial cognitive, emotional, and behavioral effects
- Scientific review: The role of hypoleptinemia in the psychological and behavioral adaptation to starvation
- YouTube: Tristyn Lee – My Experience Maintaining 4% Body Fat for 2 Years
Other hormones I have experimented with
I have experimented with a variety of other hormones, including GH, insulin, EPO, estradiol, oxandrolone, oxytocin, ADH, pregnenolone, and DHEA. I briefly discuss my experience here.
Hormones & aging
Insulin and some other hormones and their connection to the aging process are discussed here.
Strategies I follow to optimize my hormones naturally
- I optimize my sleep.
- I make sure I eat enough calories (about 3500-4000kcal per day), with enough good carbs and good fats. Whenever my caloric intake is insufficient, some of my hormones decline, including sex hormones, thyroid hormones, and IGF-1.
- I stopped any kind of fasting (both multi-day fasting as well as intermittent fasting) in part because fasting can cause all sorts of hormonal issues.
- I put a prime on exercise – but I make sure not to overdo it.
- I used to make sure that I do not dip below 14% body fat. Whenever I did, a number of hormones took a hit. Starting semaglutide allowed me to tolerate about 2% lower levels of body fat without hormonal deterioration. I now circumvent this problem altogether by taking a low dose of metreleptin sufficient to mimic a body fat percentage of about 15-20% (but without the aesthetic and metabolic downsides). The last time I checked, my body fat percentage was 10.6% (DEXA).
- I take a couple of supplements to prevent nutrient deficiencies (discussed here).
- I run an extensive hormone panel once per quarter (discuss here).
I discuss hormones & aging in more detail here.
Hormone deficiencies often go unrecognized
A non-minor number of individuals are hormone deficient. A large number of external or internal conditions can cause endocrine imbalances. These include insufficient food intake, lack of sleep, excessive exercise, fasting, ketogenic diets, low body fat percentage, immune system issues, nutritional deficiencies, high stress levels, or “healthy things done in excess”.
Quite often, people go doctor-shopping but they often cannot find anything. There are two primary reasons for this:
- The specializations and subspecializations in medicine have produced many doctors who are blind to everything out of their narrow domain and therefore hormones are rarely properly checked.
- Lab values often come back “normal” and therefore many hormone-deficient patients fly under the radar of the current medical system of doctors who just look at values that are flagged.
How to check for hormone deficiencies?
All of the major hormone deficiencies (thyroid, sex hormones, cortisol, leptin, growth hormone) have partially overlapping signs and symptoms. These include fatigue, low mood, low libido, bad sleep, brain fog, low motivation, and weight gain, and sometimes even anxiety or depression. However, these signs and symptoms are shared with many other non-hormonal conditions as well.
Because symptoms are often unspecific, getting a decent hormonal panel is a reasonable starting point.
Here is what I would test for:
- TSH, fT3, fT4 (optional: reverse T3)
- Total testosterone, SHBG, estradiol (free testosterone can be calculated from total T & SHBG & albumin)
- DHEA-S (a marker for adrenal status)
- IGF-1 (a marker for nutritional status & growth hormone secretion)
- Leptin (mostly of relevance for people with little body fat)
- Vitamin D (yes, vitamin D is a hormone as well)
Then, in combination with test results, going through the signs & symptoms of a specific hormone deficiency. Some of these signs & symptoms were listed above.
A note on blood tests
Blood tests measure what is in the blood. They do not measure cellular action, which is what it is all about. Therefore, when it comes to endocrinology, blood values matter just as much as physical signs (e.g., body hair, heart rate) and symptoms (e.g., fatigue, low libido). This was something that was hard for me to wrap my head around.
Firstly, blood tests only measure hormone concentrations at a specific snapshot in time. For example, simple things such as eating much less for a couple of days will alter hormone levels.
Secondly, blood tests do not necessarily map 1:1 to hormone action because hormone sensitivities differ between people. For example, my testosterone of 600ng/dl is not equal to your testosterone of 600ng/dl (regardless of free levels). Me and you could have different polymorphisms of the androgen receptor (AR). Or we could have different AR densities. Or we could have different versions or amounts of 5-alpha reductase (an enzyme that converts testosterone into the more potent DHT). Or we could have different versions of 3-alpha-hydroxysteroid dehydrogenase (an enzyme that converts androgens into less active metabolites). And the list goes on.
All of this makes it seem like blood tests are useless. They are not. Blood tests are highly valuable. However, one needs to keep in mind that, like any other diagnostic test, there are caveats.
It is a mystery why not much research has focused on hormone biomarkers, of which the most promising candidates are probably hormone-specific changes in certain target genes.
A note on reference ranges
Most doctors are trained to recognize only the extremes of hormone production – either “very low” or “very high”. Medical reference ranges are purely statistical ranges. By definition, 2.5% of people are below and 2.5% above are above the range.
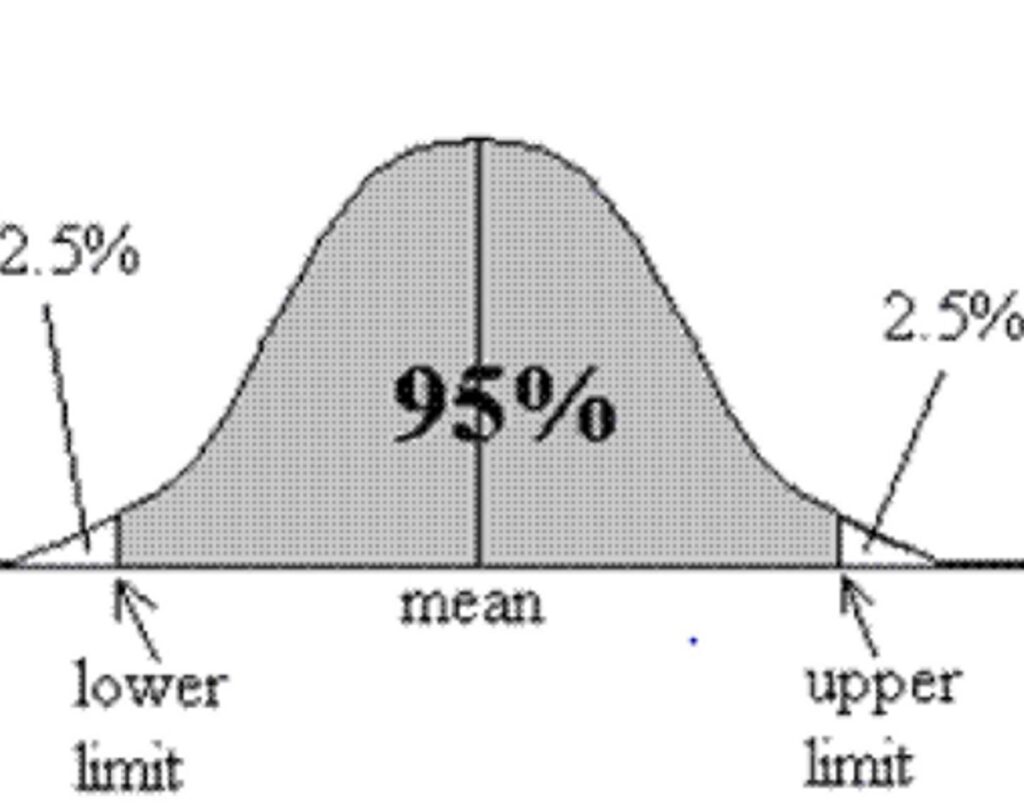
This is an issue because a lot of people who could potentially benefit from hormone replacement therapy fall into the somewhat arbitrary “perfectly normal” range, which is not necessarily the “optimal” range.
In my experience, when doctors look at my blood work, they usually treat it as an “all-or-nothing” issue. If I fall anywhere within the “normal” range, a doctor will tell me everything is great. However, if I am just slightly above or below an arbitrary number, they will tell me something is wrong.
I guess that many people who seek out doctors for problems with hormone deficiencies at their root cause do not fall below the medical reference range and thus often fly under the radar of the current medical system that just looks at values that are flagged. Their values come back “normal”. However, normal for someone 30 years their senior.
For example, the reference range of free thyroid hormones spans a range of factor three. Someone with three times as much thyroid hormone in their body will quite likely feel and function differently compared to someone with only one-third as much – despite both being considered “normal” by the conventional sick-care system.
Hormone crosstalk
The endocrine system is an intricate system. Turn one gear and many others are set in motion as well.
When one of the major hormones is modified, there are many multi-layered second and third-order effects on many other hormones. Interactions occur on many levels, including the hypothalamus & pituitary gland, other endocrine glands, the level of hepatic binding proteins, and ultimately the level of gene expression.
For example:
Thyroid hormones, IGF-1, and growth hormone are all known to stimulate other hormone axes – both at the level of the hypothalamus and pituitary gland as well as at the level of the endocrine gland. Furthermore, thyroid hormones and IGF-1 stimulate cellular activity and therefore they tend to increase the “sensitivity” of target cells to the effects of other hormones. Thyroid hormones stimulate the synthesis of binding proteins (e.g., SHBG) whereas growth hormone and IGF-1 decrease them, which may result in small changes in free hormone levels. Thyroid hormones affect aromatase activity and therefore modulate estradiol levels. Growth hormone stimulates IGF-1 synthesis, which then stimulates an enzyme called deiodinase II (which increases conversion of T4 to T3), and an enzyme called hydroxysteroid dehydrogenase type II, which inactivates cortisol to cortisone.
Analogous interactions are known for other major hormones.
These effects are just the tip of the iceberg as each of the major hormones affects hundreds of genes, and many of the molecular effects have only been roughly elucidated.
Do hormones produce “tolerance”?
The introduction of exogenous hormones is always accompanied by (some) endogenous suppression, which, however, is not the same as tolerance.
Many hormones act on gene expression, either because they act on nuclear receptors (e.g., sex steroids, thyroid hormones) or powerful cytokine receptors directly linked to transcription factors (e.g., leptin, EPO, growth hormone).
Compared to stuff that acts on G-protein-coupled receptors (the targets of most neuropharmaceuticals or recreational drugs), there is much less tolerance to these direct changes in gene expression, which is the most downstream level possible.
However, there will be some tolerance to some effects on neurotransmitter systems (which is what many people are after). For example, after starting testosterone, many experience energy, motivation, and even slight euphoria. These effects are mostly due to testosterone affecting neurotransmitter systems, particularly the dopaminergic system.
Unfortunately, changes in neurotransmitter systems and the ensuing “honeymoon period” are somewhat short-lived. After raising the dose, individuals will often “feel” much better for a short period of time (usually on the order of weeks). However, after a couple of weeks, the brain-based hedonic treadmill takes over and neurotransmitter signaling drifts back toward baseline.
Unfortunately, “how we feel” is not the best guiding factor to determine hormone dosages. “How we feel” depends entirely on the nervous system and we do not “feel” whether the liver, heart, kidney, immune system, etc. are in a hypo- or hyperhormonal state. Therefore, hormones should not be dosed solely depending on “how one feels”.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Hormone tunnel vision
If hormone levels are low, then replacing the hormone in question in a balanced way is a safe, causal, and effective way to rectify the symptoms associated with hormone deficiency. However, it seems that many people are chasing symptoms (e.g., libido, energy levels) and end up replacing hormones in supra-physiological doses even though the putative hormone deficiency was not the root cause of their symptoms in the first place.
For example, guy X might be somewhere around the 40th-50th percentile of testosterone levels. He believes he has every low-T symptom under the sun including fatigue, difficulty losing weight, poor self-confidence, low libido, etc. He is dead certain that his low testosterone levels are at fault for his symptoms and self-diagnoses with “low T”.
Guy X starts to replace his testosterone. Dopamine levels rise and he feels great for a couple of weeks. He believes that he has found the root cause. But as his dopaminergic system adapts, he is soon back to square one. Now the raise, raise, raise period begins, during which he always feels good for some time after every raise, assuming he has simply not raised his dosage enough, even though his levels of testosterone are far above the normal range already.
Gradually he starts to feel “like shit” again. Now he starts to blame the rising estrogen levels. He titrates back and forth testosterone and aromatase inhibitors, assuming he simply has not found the holy balance yet.
However, testosterone was never his issue to begin with and the initial ‘Low T’ problems come back after the honeymoon period. The issues are often complex processes in the nervous system, which might be unrelated to hormone levels. Quite often, the root cause is undiagnosed low-level dysthymia or depression (which is not the same as “suffering”).
If one’s issue is primarily of neurotransmitter or central origin, replacing hormones can definitely bring about (temporary) improvement, particularly replacing hormones in supraphysiological doses in order for them to have supraphysiological effects on various neurotransmitter systems.
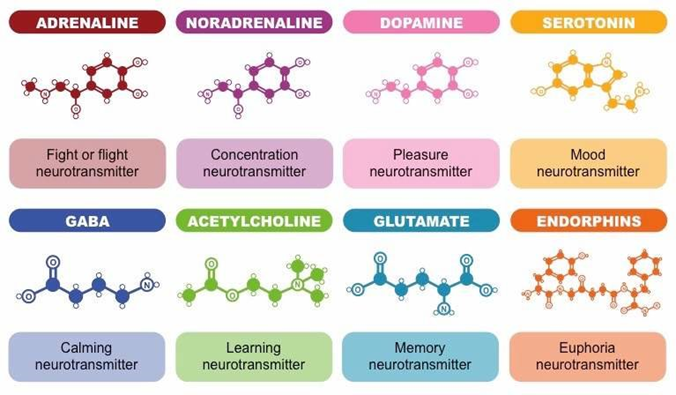
Nonetheless, in these cases, hormone replacement is not addressing the root cause and improvement will be incomplete and temporary, even though people can often feel much better over a short period of time.
Abusing hormones for symptom relief is not just unhealthy, but can be quite dangerous and cause irreversible changes in a number of organ systems. Furthermore, it is trading in short-term vitality for long-term health.
Unfortunately, the symptoms of hormone deficiencies overlap with the symptoms of low-level depression and other conditions that are only weakly related to the endocrine system.
In fact, many people with symptoms of hormone deficiencies (e.g., fatigue, low energy, bad sleep, anhedonia,) do have low-normal hormone levels. Some people choose to replace hormones, only to find that it does not bring lasting relief. The meteoric rise in TRT is just one example.
In my opinion, many people would be much better off in terms of safety, health, efficacy, and reversibility if they made major changes to their lifestyle or interfered with neurotransmission directly. For example, I know of two people who switched from testosterone replacement therapy to bupropion, with better and more sustained effects on energy, mood, motivation, and sex drive – the reason why they sought testosterone replacement therapy in the first place. Furthermore, bupropion is leaving most organ systems untouched that would be adversely affected by testosterone.
In sum, some people fare better with antidepressants. As always, the drug regimen of choice is best found through cautious empirical self-investigation.
Part V: Antidepressants (and related molecules)
Everything I think, feel, and do is mediated by brain activity. Thus, my emotions, thoughts, and outlooks are at the mercy of my neurobiochemistry and its changes. My baseline neurobiochemistry goes far beyond how I feel each moment because how I feel each moment affects the decisions I make and made, the things I do and did, and the thinking patterns I have developed over the years.
All of these then have powerful ramifications on every domain of my life and influence everything from relationships, wealth, lifestyle choices, and productivity.
Thus far I have discussed different aspects of “baseline vitality”, including the importance of sleep, diet, exercise, supplements, connection, purpose, and hormones. In this part, I will cover a bunch of molecules that have helped me to improve certain aspects of my well-being, life enjoyment, and productivity – at least while I was taking them.
A brief note on neurobiochemistry and happiness
From personal experience it became evident to me that there is a (strong) causal link between my raw biological capacity to experience happiness and the extent to which my life is felt to be worthwhile, meaningful, and exciting. If I am depressed, I am much more likely to find life meaningless. If I feel better than well, I am much more likely to find life deeply meaningful and exciting, and I am eager to get out there and do things.
Said another way, one of the major factors determining my levels of happiness is my biology. This is not my personal opinion but is well backed up by research on monoecious twins separated at birth (to correct for any non-biological factors).
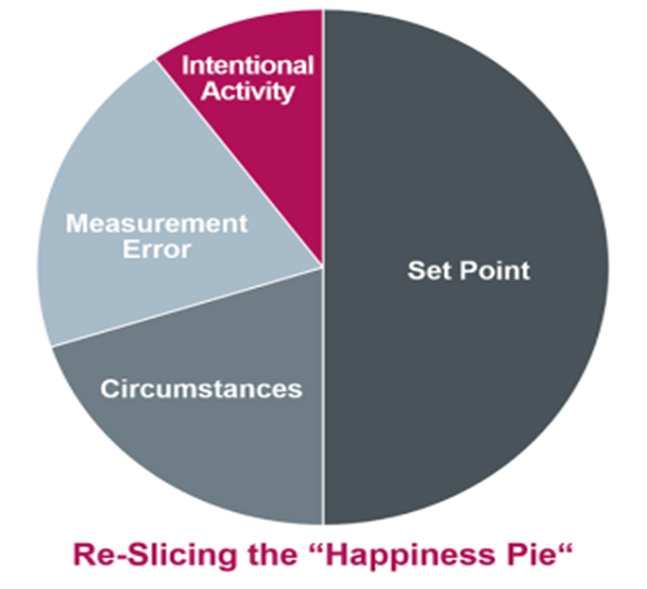
For the average human being, biological factors are as (or more) important than all of the other factors combined. However, my genes’ effect on my happiness is not by making me “happy” in the same way MDMA makes me “happy”. The effects on my happiness are much more indirect.
As mentioned in the section on guiding principles, my biological factors ripple through my life in the same way an earthquake ripples through the Earth’s crust.
Genes influence my neurobiochemistry. My neurobiochemistry then not only affects my moment-to-moment well-being (the way I “feel” on a daily basis) but also my thinking patterns, the way I act, and therefore my life overall: relationships, wealth, relationships, status, profession, etc. — which all have independent effects on my happiness levels.
My biological “set point” (including my levels of neurotransmitters as well as a number of genes and some other poorly understood biological factors) co-determines many of my personality traits, my capacity to do work, my level of motivation and drive, my thinking patterns, my general level of my (biochemical) well-being, and how my life unfolds in general.
Obviously, there are other crucial factors such as parenting style and early life experiences, but biology usually gets the short end of the stick despite probably deserving the longer end.
The power of neurobiochemistry
Most individuals are very vital – even hypomanic – as kids. Usually, children have boundless energy, are motivated, curious, enthusiastic, capable of feeling profound feelings, and have big goals and dreams.
Over time, “vitality” usually quiets way down. While many blame our archaic education system or Groundhog Day setting in, I argue that this is mostly a neurobiochemical shift from child-like hypomania to a more “normal” state. Among other poorly understood changes at the level of gene expression, neuroplasticity, and neurotransmitters, the nervous system becomes gradually less “overflowing”.
This hypothesis is supported by the fact that bipolar individuals who transition from “normalcy” into hypomania or mania usually re-experience this child-like state of intense vitality. And very often, thoughts and outlooks follow suit. People who were “meh”, bleak, or dreary are suddenly full of purpose and meaning even though their life situation or mindset did not primarily change.
From personal experience I can say that it is, to some extent, possible to recreate, or at least approximate, this state (and without having to rely on stimulants).
I discuss this in more detail here: The Power of Neurobiochemistry
We get used to new states quite quickly
After experimenting with lots of neuropharmaceuticals I found that, for me, after a couple of days to weeks, it always seems like “it has always been this way”. Most of my friends report the same.
For example, during a depressive episode, one friend was sure that it would always stay this way and that it would never get better. After a couple of weeks on escitalopram, she could barely relate anymore and the depressive episode seemed like a distant dream. That humans get used to new states of mind quite quickly seems to be a common theme.
A brief note on neurotransmitters
There are a variety of neurotransmitters. Among the most powerful of these are the three major monoamine transmitters: serotonin, dopamine, noradrenaline.
Very simplistically:
Every individual has a certain baseline level of these neurotransmitters, which is mostly determined by genetics (over 50%), hormones, and lifestyle.
I will now discuss some of these transmitters in a little more detail.
- Dopamine has to do with excitement and motivation and a lack thereof is associated with listlessness, apathy, and anhedonia. Dopamine feels like “I want to have this, and I am excited to get it”. For example, when I am sitting in front of my favorite food after 24 hours of fasting.
- Noradrenaline has to do with alertness and a lack thereof is associated with lethargy and exhaustion. Noradrenaline feels like “energy”. For example, when I go into a cold shower.
- Serotonin is the most complex of the monoamines. Very simplistically speaking, serotonin has to do with calmness and contentment, and a lack thereof is associated with low self-confidence, guilt, and rumination. Serotonin feels like “inner warmth”. For example, when I am practicing gratitude.
Obviously, these descriptions are severe simplifications. I discuss these and other neurotransmitters in much more detail here: An Introduction to Neurotransmitters
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
A brief note on antidepressants
Antidepressants are much more than “a pill to feel well”.
On the biological side, most antidepressants increase one or more monoamine transmitters, stimulate neurogenesis within the hippocampus, and lead to a host of adaptive changes between and within neurons, including receptor reregulation and changes in gene expression.
On the non-biological side, antidepressants affect moment-to-moment well-being, thinking patterns, and behavior, all of which do not just affect a person’s “inner” life, but also a person’s “outer” life, which then has a separate effect on a person’s feelings and thoughts – beyond the direct effects of the medication.
I discuss this in more detail here: What Kind of Antidepressant Should I Choose?
Related articles:
Experience reports
They are arranged approximately based on the amount of value I derived from them.
- Semaglutide (& appetite regulation)
- Moclobemide (& MAO inhibitors)
- Low-dose psychedelics (“microdosing”)
- High-dose psychedelics (“tripping”)
- Vortioxetine
- Bupropion
- Ketamine
- L-theanine
- Ibuprofen
- Low-dose naltrexone (LDN)
- Tianeptine
- Antipsychotics & mood stabilizers
- Is it safe to take stimulants and antidepressants forever?
- Thoughts on modern psychiatry
- Case reports: Examples of cases that are hard to treat
Semaglutide
Semaglutide is a GLP-1 agonist and one of my favorite drugs. It was originally developed as an antidiabetic agent because GLP-1 amplifies glucose-induced insulin release. However, as its powerful weight-loss benefits became evident (which go far beyond simply reducing appetite and energy intake) trials for obesity started.
Lo and behold, at the highest dose, people lost about 18% of their body weight in the first year. It was soon patented as an anti-obesity drug. The anti-obesity drug.
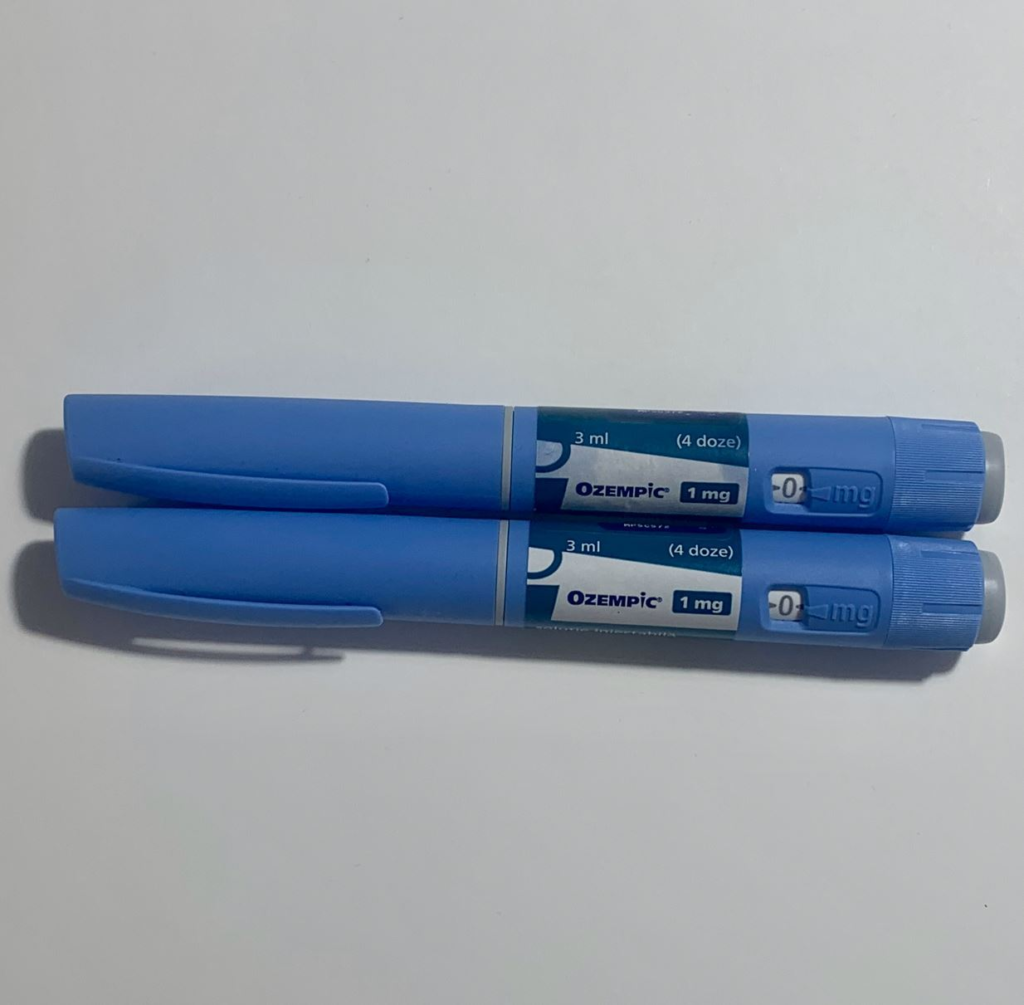
It did not take awfully long before it started to be widely used (and abused) as a weight-loss agent, both on and off-label. Given that we have patient data on GLP-1 agonists since 2012, major negative unintended long-term side effects seem unlikely.
I predict that in 10 years a double-digit percentage of the population will be on a GLP-1-agonist or analogous drugs (if the world as we know still exists by then, which is far from certain).
The reasons I have included semaglutide in the section on “antidepressants and other molecules for enhancing well-being” are multiple:
- It is an awesome drug, and it helped me out a great deal.
- Hacking my appetite and weight improves my vitality and looks, both of which are crucial to my well-being.
- Taking semaglutide is like sending a constant satiety signal to my brain. By reducing appetite and therefore distractions, for me, semaglutide is useful for productivity and “nootropic” purposes.
- In the past, I struggled with getting lean and staying there. Consequently, a lot of my time & energy was wasted on thinking about food. Brainpower that could be used for other things, for example improving myself and the world.
- GLP-1 agonists do not just help with food addiction but their anti-addiction/anti-craving effects seem to be more broad. Anecdotally, they seem to help some people with all kinds of addictive behaviors.
It is surely no coincidence that many top performers use semaglutide, the best drug currently available to reduce the human natural tendency to overindulge.
I discuss semaglutide, and my experience with it, in more detail here.
Moclobemide & MAO-inhibitors
Moclobemide is a poorly known all-rounder. It boosts energy levels, mood, sleep, and hormones. On the therapeutic side, it helps with anxiety, obsessive-compulsive symptoms, depression, a lack of energy, and ADHD symptoms, all while not blunting emotions, worsening libido, or dysregulating appetite.
I always thought there has got to be something out there that makes me feel and perform better than baseline. Short of lifestyle hacks and hormone optimization, the only thing that really worked for me (n=1), was a low dose of moclobemide. However, even moclobemide had some downsides, in particular a slight emotional and cognitive blunting.
Moclobemide is neither widely known nor widely used. While it is not even available in the US, it is a first-line antidepressant in Australia and some northern European countries.
I heard that some cyclists use moclobemide during the Tour de France because it does not show up in any drug screening (unlike most stimulants).

I discuss moclobemide, and my personal experience with it, in more detail here.
Low-dose psychedelics (“microdosing”)
We are currently undergoing a psychedelic renaissance. The number of people who use psychedelics for self-improvement purposes is rapidly growing by the day. Taking low doses of psychedelics (“microdosing”) can enhance creativity, boost physical energy levels, increase emotional well-being, and promote mental flexibility. A non-minor number of people also claim that microdosing helps them with anxiety, depression, and addiction.
I discuss microdosing in more detail here.
High-dose psychedelics (“tripping”)
For thousands of years, various psychedelic molecules have been in use by different human tribes all over Earth. Western culture has only recently noticed their potential, though they had been an “open secret” among intellectuals and scientists for a long time.
At higher doses, psychedelics quite reliably cause mystical-type experiences, which can be subjectively incredibly meaningful. In a clinical study, 80% of people that were given a large dose of psilocybin rated it as one of their most meaningful – sometimes even the most meaningful – experiences.
A single of these mystical-type experiences can stimulate users for weeks and months – although the stimulation is not “bottom-up”, as is the case with most biological interventions, but rather “top-down”.
Aldous Huxley advocated the use of LSD “to make this trivial world sublime,” and reportedly even took the drug on his deathbed.
While responsible use of psychedelics has many upsides (e.g., long-lasting positive attitude adjustments, a renewed sense of wonder, greater joy for life, helping users to find purpose), psychedelics are not toys and there are also significant risks. In the worst case, they can trigger psychosis, cause PTSD, or induce HPPD – all of which are discussed shortly.
I discuss psychedelics in more detail here.
Vortioxetine
Vortioxetine is an SSRI – though not a classical one. It is the newest SSRI brought to market. Even though people’s reactions to drugs differ, the unique properties of vortioxetine make it, in my opinion, a decent choice as a first-line antidepressant.
Even though it has similar side effects to other SSRIs, these seem to be of lesser magnitude. It has a less severe effect on sexual function, less emotional blunting, less weight gain, and a lower incidence of insomnia.
Uniquely, vortioxetine seems to have nootropic effects that are thought to be somewhat independent of its antidepressant effects (and its manufacturer Lundbeck did an excellent job at marketing that). However, whether that is true or clinically relevant is currently not fully known.
The major downsides are that it is not very effective at treating anxiety and its price is high –
it is still patented and is therefore quite expensive.

I discuss vortioxetine, and my experience with it, in more detail here.
Bupropion
Large parts of the population in Western countries currently consume either alcohol, cigarettes, weed, or toxic amounts of sugar – or a combination of these. Millions of others consume amphetamines, opioids, and cocaine. These drugs provide temporary pleasure, but almost always have negative long-term consequences.
Viewed in terms of mortality, morbidity, or even life enjoyment, people would be better off if they switched to “good drugs”, namely drugs that have long-term beneficial effects on the user. In my opinion, bupropion may be such a drug.

Bupropion is a much milder (but much more sustainable) version of amphetamine. It has powerful mood-brightening effects, is stimulating, increases drive, boosts libido, decreases appetite, and has few adverse effects once the initial accommodation is over.
Bupropion is an atypical antidepressant that mainly works on the noradrenergic and dopaminergic systems while leaving the serotonergic system mostly untouched.
Bupropion is the only frequently prescribed antidepressant that does not cause weight gain, sedation, or sexual dysfunction – quite the opposite, it tends to improve energy levels, sexual function, and tends to cause weight loss. It also has a milder withdrawal than many other antidepressants.
Perhaps unfortunately, bupropion is rarely used as a first-line antidepressant because many physicians assume that it worsens anxiety. Contrary to popular belief, bupropion is no more likely to worsen anxiety than SSRIs, other than perhaps during the first weeks or so. Furthermore, there is even preliminary evidence that bupropion may be an effective treatment for generalized anxiety disorder and social anxiety disorder (without depression).
For some reason, bupropion is a controlled substance in Russia.
I discuss bupropion, and my experience with it, in more detail here.
Ketamine
A good friend of mine has recurrent episodes of depression. Whenever depression is looming, he feels hopeless and helpless. Even though he knows exactly what is happening (he is a doctor), what he feels takes over. According to him, a single injection of ketamine is the only thing that reliably gets him out before the depression gets worse.
Ketamine has been used for anesthetic purposes since the 1970s. For recreational purposes, “Special K” is abused throughout the world, especially in Southeast Asia and the UK. However, at lower than anesthetic or recreational doses, ketamine has some unique and interesting properties.
Currently, in psychiatric wards all over the world, there is a lot of talk and hype about using ketamine to treat a variety of conditions, especially deep biological depression. Taken at around 1/10th of an anesthetic dose, it rapidly lifts mood, abolishes suicidal thoughts, bans anxiety, and even improves obsessive-compulsive symptoms – at least for a subset of patients.
Compared to other drugs, ketamine exerts its effects not until after the drug has already left the system. Furthermore, the effects are “natural”, in the sense that the balance of monoamine neurotransmitters is not distorted.
While single-use ketamine is known to improve well-being, energy levels, and cognition for about 1-2 weeks (and more rarely months), repeated-use ketamine, a so-called “ketamine series”, is thought to bring about powerful neuroplastic changes.
The main benefit of ketamine is a rapid reduction in depressive symptoms, particularly suicidal ideation. The primary concerns regarding ketamine are its often temporary benefits and its potential neurotoxic effects, which may be of relevance at even therapeutic doses.
I discuss ketamine, and my personal experience with it, in more detail here.
L-Theanine
L-theanine is a non-proteinogenic amino acid that is synthesized by a couple of fungi and plants, among them tea. It is an analog of glutamate, an excitatory neurotransmitter. It is known for its ability to promote relaxation without inducing drowsiness, as well as its potential cognitive benefits.
In the nootropic community (if that is even a thing), it is most famous for being combined with caffeine to cancel out some of its adverse effects while promoting cognition.
In addition, some people find that L-theanine by itself is a useful short-term anti-anxiety agent – without the risks and side effects of benzodiazepines. Because little to no money can be made from it, pharmaceutical companies have little interest in generating the evidence necessary for it to be more widely employed for clinical use.
I discuss L-theanine, and my personal experience with it, in more detail here.
Ibuprofen
Certain subtypes of lethargy or depression are due to sickness behavior. “Sickness behavior” refers to a set of behavioral and mental changes that occur in response to an infection or inflammation.
Sickness behavior is characterized by a range of symptoms, including brain fog, fatigue, lethargy, anhedonia, a desire to withdraw, and altered sleep and appetite. These changes are thought to be an evolutionary adaptation that enables the body to conserve energy and focus on fighting infection or inflammation. Furthermore, it is thought that “sickness behavior” also induces a withdrawal from group living, which would help the group as well as prevent ostracization of the individual.
Infections occur more or less frequently in everybody, depending on the strength of one’s immune system and exposure to viral pathogens. Many of these infections are too minor to manifest in true “sickness” (and may therefore go unnoticed) but large enough to decrease vitality in major ways.
Therefore, certain instances of unexplainable drops in energy levels, mood, motivation, and cognition, are due to (unrecognized) inflammation. Potent cytokinemia is a multiplier-by-0 (x*0 = 0) for good energy levels and mood, and stimulants are inadequate to address this.
In this regard, anti-inflammatory drugs of the NSAID class can boost energy & mood in certain situations.

I discuss ibuprofen, and my experience with it, in more detail here.
Low-dose naltrexone (LDN)
Naltrexone is a potent opioid receptor antagonist. In the clinical setting, naltrexone is sometimes prescribed for opioid or alcohol dependence, specifically to block the feeling of “pleasure” and to reduce “cravings”.
However, given at extremely low doses, about 1/50th to 1/10th of clinical doses, low-dose naltrexone (LDN) has a couple of interesting properties. LDN seems to modulate a variety of systems, including the reward system, hypothalamic subsystems, and the immune system.
Potential benefits range from helping with all kinds of addictions (including behavioral addictions), low libido, fibromyalgia and other pain states, chronic fatigue syndrome, burnout, and low-level inflammation. However, it remains to be seen whether LDN is more hope than hype.

I discuss naltrexone, and my personal experience with it, in more detail here.
Tianeptine (& opioids)
Tianeptine is an atypical antidepressant. It is mood-brightening, activating, increases motivation, deepens emotions, and is a powerful anti-anxiety agent. Some people (ab)use it as a nootropic.
I discuss tianeptine, and my personal experience with it, in more detail here.
Antipsychotics & mood stabilizers – Their potential off-label usefulness (?)
Even though I have never tried any of them, I will now briefly discuss antipsychotics, mood stabilizers, and similar drugs as far as they may be useful for the treatment of “normal” mental disorders (non-psychotic states).
I discuss antipsychotics & mood stabilizers in more detail here.
Is it safe to take stimulants and antidepressants forever?
Neuropharmaceuticals do not only change brain function acutely (i.e., as long as they are in the system) but also have long-term effects on brain structure and brain function – and some of these changes are irreversible. Because this article is already very long, I touch on this topic in much more technical detail here.
Thoughts on modern psychiatry
Mental health is the strongest predictor for life satisfaction and explains twice as much as the second strongest factor (physical health). Given that the human brain creates every aspect of human experience, unfortunately, most but not all psychiatrists I have met knew disturbingly little about brain biology.
Many just seemed to follow blindly what they were taught by their seniors. Furthermore, many seemed to be somewhat detached from other disciplines, therefore blind and deaf to everything that is not “mental”, such as lifestyle, hormones, metabolic health – and how these influence the brain & mind.

I share my thoughts, criticism, and personal experience with modern psychiatry in more detail here.
Case reports – Humans are complex
Even though there are many different avenues for biological intervention, there are many individuals that are hard – if not impossible – to treat. The following examples should illustrate how complex things can be. Often, it is not as simple as doing A, B, C, or taking X, Y, Z.
The case reports below only deal with the biological side of things. It is important to note that not every energy and mood-related problem can be attributed to a “brain disease” or primarily biological factors. With the following case reports I aim to demonstrate the complexity of things.
Some of the following examples were inspired by people I know, some by people I have read about, and others are entirely fictional.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
Case A
A was a happy and energetic child but now she has problems with sleep, depression, and anxiety – despite being already on the highest therapeutic dose of escitalopram. A has taken a lot of MDMA in her early adulthood.
While the first couple of times were magic, it took her progressively longer to recover, until she did not anymore. An MRI scan shows no signs of pathological changes (but the degeneration of serotonergic nerve endings cannot be seen).
Case B
B always feels tired, cold, cannot lose fat, and has low energy levels. B has a mild form of panhypopituitarism due to an unrecognized traumatic brain injury as a child, which injured the axons making up the pituitary stalk.
He would benefit from the replacement of multiple hypothalamic hormones, though his doctors never bother to look at them properly because they all came back in the low “normal” range.
Case C
Throughout his childhood, C was anxious and socially awkward. Even though he has now got a decent group of friends, the feeling that “something is missing” does not quite leave him. Unbeknownst to him, his mother was under major stress during pregnancy.
Consequently, the high levels of glucocorticoids exerted a disproportionately major influence on his brain wiring. Among other things, hypercortisolism led to significant differences in the cytoarchitecture and connectivity of his amygdalae, prefrontal cortices, anterior cingulate cortices, and insulae. These differences will persist throughout his life.
Case D
D is impulsive, anxious, and prone to rage. To help him with wrestling in high school, D had dabbled in anabolic steroids. Not only did they stunt his growth, but certain emotional brain centers had wired differently compared to what they would have. Now he is permanently stuck with a “hyper-male” brain. And a hyper-hairy body.
Case E
E has a severe form of atypical depression, characterized by low energy levels, hypersomnia, and weight gain. For unexplainable reasons, the activity of his glutamatergic and monoaminergic systems has settled into very low attractor states and defies conventional treatment. Unfortunately for him, MAO inhibitors are not something most doctors are comfortable with, and therefore he never gets to try them.
Case F
Throughout his adolescence, F did so much exercise that he was constantly sore. Even though the underlying structural and chemical damage has long been repaired, F has focused so much on the pain that the neurons and connections responsible for pain transmission have hypertrophied and strengthened respectively. He is now stuck with chronic pain that is “mostly in his head”.
Case G
G has taken SSRIs and reacted badly to them. After only a couple of days, he developed genital numbness, anorgasmia, anhedonia, and lethargy. Even after stopping, symptoms lingered on. He educated himself and tried out dozens of different treatments on his own to no avail because his symptoms are caused by stubborn changes in gene expression complicated by serotonergic toxicity.
Case H
H is plagued by depression, anhedonia, a lack of motivation, and thought loops. All of these symptoms can be traced back to a time when H smoked weed a couple of times during a sensitive period of brain development. This has resulted in widespread aberrant synaptic pruning.
Case I
Case I had severe childhood trauma, and the consequences still pervade monoaminergic systems, neuroendocrine regulation, and psychological well-being. Even MDMA-assisted psychotherapy did not help.
Case J
J has structural aberrances in the basal ganglia systems due to genetics & “bad luck” during intrauterine development. He is plagued by debilitating thought loops, obsessive tendencies, and impairments in executive functions. Stimulants help for a bit but eventually they “poop out”.
Case K
K is always tired, anhedonic, and prefers to stay by himself. Conventional treatment with several antidepressants was unsuccessful because the underlying problem is an unrecognized autoimmune disorder, which induces sickness behavior due to chronically elevated cytokine levels.
Case L
L is a rationalist and nihilist. After reading the wrong kinds of philosophy, he has successfully trained his neural wetware to use negative and pessimistic thinking patterns. He responds well to bupropion but “blames” his biology for his newfound zest for life and successfully uses reason to subdue any positive emotion. To him, everything is pointless anyway, and the multiverse is an apathetic, cold, and dark place. He stops the bupropion long before new thinking patterns can engrain themselves.
Case M
M’s energy and mood are notoriously difficult to treat. Unbeknownst to her, because of natural variation, she has a significantly lower number of catecholaminergic neurons and adrenergic nerve endings than most people.
Case N
N is constantly drained and zombie-like fatigued. He has tried a lot of different pharmaceuticals and lifestyle interventions, but things do not seem to get better. Unfortunately, nobody has recognized his sleep apnea.
Case O
O suffers from chronic fatigue due to long-COVID. He is treated with stimulants, which help little. Unfortunately, he never learns about immunosuppression, immunoadsorption, or b-cell depletion, which would help him because his fatigue is in part brought about by autoantibodies against endogenous muscarinic and beta-adrenergic receptors.
Summary
Diagnosing as well as treating certain issues can get quite complex quite fast.
Part VI: Stimulants
One of the most important habits to achieve things in life is to do the hard things and to repeatedly take action. However, my desire for doing the hard things or taking action is in part regulated by dopamine levels, whereas my ability to do so is partly a function of energy levels.
For example, for me, procrastination mostly happens whenever I am low energy, such as after a bad night’s sleep. If I then take a stimulant, the half-assing is gone quite fast. If I improve energy levels and/or dopamine, I simply start to do. In this way, stimulants allow me to get “more” out of my brain and body than what would otherwise be possible.
Furthermore, my need for food and sleep is reduced, while concentration and cognition are improved. This is one of the main reasons I turn to pharmacological crutches of the stimulant class occasionally. Far more powerful than self-help books.

The dark side of stimulants
When I was younger, I thought that eliminating periods of listlessness or tiredness would vastly improve my productivity, impact, and applied intelligence. While I still believe this, stimulants were not a viable way to get there (and more importantly, to stay there).
Millions of people around the world (ab)use stimulants on a daily basis. Caffeine is just one example. While the benefits are numerous, such as increased energy levels, better mood, improved cognition, appetite suppression, etc., the downsides of stimulants are rarely discussed – in many cases not even by the doctors who prescribe them.
Although stimulants do have their usefulness, and I have used them a lot myself, my fondness for them has steadily diminished over time.
On stimulants, whether it is modafinil, methylphenidate, or amphetamine I partially lose my metacognition and I become autistically glued to whatever I am doing. Then, I find it hard to thoroughly think stuff through and to judge whether I am working on the right things because everything becomes salient. While this is fine for working on boring stuff, this is not conducive to living a balanced life.
Furthermore, I and many other people had to learn the hard way that prolonged stimulant use can cause an impairment of multiple neurotransmitter systems – especially the dopaminergic system.
As I was using stimulants more frequently, I did not fully realize the situation I was in because my use was keeping neurotransmitter levels artificially elevated. It was not until I came off that I realized how dysfunctional I had become at baseline.
I jumped back on in order to avoid the nasty withdrawal symptoms. This caused me to keep using the stimulant in question for prolonged periods of time, at ever-increasing dosages, without ever allowing my brain to rest and recover. The stimulant I am talking about is caffeine (discussed shortly).
Luckily, for me, the cycle of physio-psychological dependence did end well. I recovered quickly. However, I have met several people who did not recover from having used harsher stimulants of the amphetamine class. Depression, burnout, fatigue, and anhedonia often last for a long time after.
It is my opinion that if the factors discussed in earlier sections are taken care of, the vast majority of people do not need stimulants. In fact, I sincerely believe that, for most people, using stimulants more often than very occasionally is more harmful than beneficial. Obviously, there are exceptions, but most people are not them if lifestyle and hormones are taken care of. Unfortunately, about 5-10% of people in Western countries are using prescription stimulants to function.
In the following section, I discuss a variety of different stimulants, my experience with them, and my overall thoughts and opinion.
Three brief notes
A brief note on nootropics
Nootropics, or “cognition enhancers”, are taken with the intent to enhance cognition. Ideally, a nootropic agent improves alertness, working memory, memory recall, inhibitory control, attention span, selective attention, and reasoning.
At low therapeutic doses, almost any stimulant has nootropic effects. However, there are nootropic molecules that are not stimulants, such as creatine, vortioxetine, tianeptine, or L-theanine.
- Some of these non-stimulant nootropics are discussed in Part V.
- Herbal nootropics are discussed here.
- In my opinion, the best “nootropic” is general health, hormones, and a good lifestyle, which is discussed in Part II.
- I discuss the topic of intelligence enhancement in more detail here.
A brief note on depression
When I was depressed, I was devoid of energy, motivation, and drive. Furthermore, depression worsened my cognition in pretty much all aspects. For example, it was hard to think logically, make good decisions, be creative, or remember things.
Even though antidepressants are not conventional stimulants, one problem to which, in my opinion, “authorities” on nootropics and stimulants do not give enough emphasis, is the complex interplay between energy levels, mood, and cognition.
Therefore, for me, taking an antidepressant was a better nootropic and stimulant than stimulants. Depression is discussed in more detail here:
A brief note on substance abuse
“In most cases, the issue does not amount to drugs vs. no drugs, but rather to allowing people to opt for better ones.” Philosopher David Pearce uses the term „good drugs“ to describe molecules that not only improve subjective well-being but also contribute positively to one’s life in a way that makes ethical and material sense.
A large number of people are addicted to what David Pearce would call “bad drugs”. In this regard, I will also discuss THC, methamphetamine, MDMA, and cocaine, as well as molecules that might help with withdrawal and coming off.
How stimulants work: A quick primer
Stimulants, as their name suggests, are molecules that stimulate the nervous system. Most but not all work by directly or indirectly enhancing catecholamine signaling (dopamine and/or noradrenaline).
Stimulants increase alertness, mood, the ability to focus, incentive salience (motivation), task salience (making boring stuff more fun), vigor, sociability, libido, motor activity, muscle function, and suppress appetite. In high doses, stimulants also recruit opioidergic pathways and produce euphoria, which makes them common drugs of abuse.
Stimulant principles for responsible use are discussed in more detail here.
Subscribe to the Desmolysium newsletter and get access to three exclusive articles!
In general, (most) stimulants exert their effects through a combination of two things:
- #1 Stimulants increase energy levels: More specifically, they increase the baseline activity of the central nervous system – usually by directly or indirectly elevating levels of noradrenaline, histamine, and glutamate. This is quite performance-enhancing in itself.
- #2 Stimulants increase motivation & cognition: More specifically, many but not all stimulants also increase dopamine, which increases focus, motivation, and cognition regardless of energy levels.
I discuss these neurotransmitters in more detail here: An Introduction to the Science of Neurotransmitters.
Table of contents
They are arranged approximately based on how often I used them. I am sure that, in retrospect, some (and perhaps even most) of them did more harm than good, particularly stimulants from the amphetamine class.
- Nicotine
- Modafinil
- Caffeine
- Ephedrine
- Selegiline
- Hydrocortisone
- Methylphenidate
- Amphetamine
- Lisdexamphetamine
- Reboxetine
- Midodrine
- Racetams
- THC
- Noteworthy molecules stuck in pharmaceutical pipelines
Nicotine
Nicotine is unfairly demonized because it is the active ingredient in tobacco, which is responsible for about 6 Mio. deaths per year worldwide, 25% of which are from cancer, 25% from COPD, and 50% from cardiovascular diseases. In fact, it is thought that about 30% of cancers and 90% of COPD are attributable to smoking.
Even though addictive, nicotine itself is thought to be quite safe. It is a weak stimulant and a great nootropic. It is also thought to protect against dementia, particularly Parkinson’s disease.

I discuss nicotine, and my personal experience with it, in more detail here.
Modafinil
Modafinil is used off-label by a lot of students, workers, scientists, and professionals that require and desire peak alertness, and for many of them, modafinil is the perfect stimulant and cognitive enhancer.
Modafinil improves wakefulness, motivation, task salience (the ability to work on boring things without finding them boring), memory formation and retrieval, selective attention (though perhaps at the expense of creative thinking), and some other aspects of executive functions. All while having little abuse potential, crash, or side effects.
Its US approval was partially funded by DARPA, a US agency responsible for researching new military technologies, in order to provide troops with a non-addictive and less crash-prone alternative to amphetamines during long and exhausting missions. Modafinil is approved for the treatment of narcolepsy but is often used as an augmentation agent in a wide range of disorders such as cancer, depression, ADHD, and chronic fatigue syndrome.

I discuss modafinil, and my personal experience with it, in more detail here.
Caffeine
Coffee is the second most traded resource in the world, mainly because a large share of the population is addicted to caffeine. In the Western world, over 75% of adults drink caffeine-containing beverages daily.
When caffeine was introduced to the Western world, a lot of people started consuming it widely. Some historians argue that caffeine contributed significantly to the speed and extent of the scientific revolution, in part because people switched from drinking alcohol to drinking coffee, with significant societal impacts.
Caffeine has been in widespread use for over 200 years, and it was the only stimulant widely available until the 20th century. This makes caffeine also one of the most widely researched exogenous molecules overall. Consequently, we have truckloads of data showing that caffeine is quite safe for life-long consumption.
When it comes to mind-altering substances, caffeine is an outlier. Its use is socially acceptable almost everywhere in the world (except for Mormons). Most people do not consider caffeine a “drug” in the same way that ethanol is socially acceptable and not considered a “drug” – though mammalian physiology could not care less about our arbitrary social acceptance.
I discuss caffeine, and my personal experience with it, in more detail here.
Ephedrine
Ephedrine is a naturally occurring alkaloid found in the ephedra plant and structurally resembles adrenaline. It has been widely used in TCM, Ayurveda, and Southeast Asia for about 3000 years for a variety of conditions.
Before the year 2000, ephedrine was widely sold and used as an over-the-counter stimulant and weight-loss agent in the US and Europe. It was frequently combined with caffeine in the so-called EC stack in pre-workouts, appetite suppressants, and fat burners.
However, as more and more people started to use ephedrine for the synthesis of methamphetamine, its sale was swiftly restricted. In most countries, it is currently available only on prescription or behind the counter.
A little bit of history. At the close of the 19th century, the company Merck wanted to find a new asthma treatment. Ephedrine was a known bronchodilator and so researchers played around with chemically manipulating it. Amphetamine and methamphetamine were born.

I discuss ephedrine, and my personal experience with it, in more detail here.
Selegiline
Selegiline is an irreversible MAO-B inhibitor. In other words, it destroys the enzyme that breaks down dopamine and some trace amines. Selegiline was developed for the treatment of Parkinson’s disease. More recently, a transdermal patch (Emsam) was approved for the treatment of depression. Some people use selegiline as a cognitive enhancer because it elevates dopamine levels in a unique way.

I discuss selegiline, and my personal experience with it, in more detail here.
Hydrocortisone
Hydrocortisone is the pharmaceutical version of the hormone cortisol, the so-called “stress hormone”. Cortisol is discussed in the section on hormones.
Cortisol gives energy, vitality, and “punch”. Cortisol clarifies thinking, sharpens concentration, and improves cognition & memory, giving a “clear” head and a sharp mind. Furthermore, cortisol increases the availability of plasma nutrients and regulates the immune system. All of this makes physiological and evolutionary sense in times of stress and danger.
While cortisol excess has degenerative effects on every bodily tissue, cortisol deficiency makes people feel miserable, including brain fog, abysmal energy levels, “feeling like shit”, and weakness. Replacing it in a cortisol-deficient person has quick and dramatic effects. Therefore, hydrocortisone is thought to be a viable option for the (temporary) treatment of burnout states, and chronic fatigue syndrome.
Furthermore, the use of corticosteroids can help atypical depression and kinds of depression that are due to “sickness behavior”. However, hydrocortisone is powerful, and its use can be quite dangerous, degenerative, and pro-aging.

I discuss hydrocortisone, and my personal experience with it, in more detail here.
Methylphenidate
Methylphenidate (Ritalin) is the prototypical ADHD drug and in most countries (other than the US) it is usually the first-line treatment for ADHD (and to “slow down” hyperactive children).
At therapeutic doses, it increases focus, alertness, and concentration, while decreasing impulsivity. Moreover, due to its potent dopaminergic properties, methylphenidate is an effective (but somewhat underused) augmentation agent in the treatment of depression.
MPD has low oral bioavailability (30-50%) and a duration of action of only about three hours. Therefore, it is often taken in an extended-release form.
I discuss ADHD and my thoughts on it here.
I discuss methylphenidate, and my personal experience with it, in more detail here.
Amphetamine
Amphetamine (“Adderall”) is the prototypical stimulant. It has been created in the late 1880s and throughout its existence it was medically prescribed for a vast number of conditions, including ADHD, obesity, lethargy, depression, and impulse control disorders such as pathological gambling or binge eating.
Adolf Hitler is thought to have begun using amphetamine occasionally after 1937 and to have become eventually addicted to it in the early 1940s. A vast number of soldiers were using it as well. Were it not for amphetamine, WWII may have perhaps played out quite differently.

At present, millions of individuals diagnosed with ADHD take amphetamines on a daily basis. I share my thoughts on ADHD and its treatment here: ADHD- To Treat Or Not To Treat?
Adderall is in a sense similar to anabolic steroids. Online anecdotes tend to paint a “great cheat code for life” picture. However, that picture is very misleading and does not really capture the whole storyline. Lots of cheerleading first-time users that stop documenting their downfall seem to be a common theme.
I discuss amphetamine, and my personal experience with it, in more detail here.
Lisdexamphetamine
Lisdexamphetamine (Vyvanse) is the new kid on the block and in recent years its use has become rampant among many parts of the population (particularly in the US).
Lisdexamphetamine is a prodrug of dextroamphetamine. Compared to instant-release amphetamine (Adderall), it has a smoother onset and offset, less abuse potential, and slightly fewer side effects. Nonetheless, coming off is just as hard, and (potential) adverse effects on long-term brain health may be the same.

I discuss lisdexamphetamine, and my personal experience with it, in more detail here.
Reboxetine
Reboxetine is a noradrenaline reuptake inhibitor (NRI). It is used as a non-stimulant alternative in the treatment of ADHD and as an augmentation agent in the treatment of depression. It has also shown promise in treating panic disorder.
Atomoxetine (a chemical cousin of reboxetine) is pretty much the same, though also has a slight affinity for the serotonin transporter (SERT).
I discuss reboxetine, and my personal experience with it, in more detail here.
Midodrine
Midodrine does have no stimulant effects whatsoever, and still, it can abolish certain instances of “fatigue” and brain fog. Sometimes and for some people, bouts of weakness, lethargy, and brain fog are due to hypotension (low blood pressure) – especially after intense exercise.
However, for people that do not measure their blood pressure regularly, it is almost impossible to distinguish whether weakness, listlessness, and brain fog are due to low blood pressure or other kinds of fatigue such as sleepiness.
Whatever the case, people are tempted to drink coffee or take other stimulants even though in the case of low blood pressure being the issue, it may be more effective to use vasopressors, such as midodrine or etilefrine, instead of central nervous system stimulants.
I discuss midodrine, and my personal experience with it, in more detail here.
Piracetam
There seems to be an underground community of people who guineapig with a large variety of unregulated and under-studied Eastern-bloc molecules, including various racetams, noopept, selank, semax, and bromantane. The mechanism of action of none of these is fully known, and neither is their safety.
Piracetam, a nootropic drug given to dementia patients, and levetiracetam, an anticonvulsant, are two racetams that have been studied more thoroughly.

I discuss racetams, and my personal experience with them, in more detail here.
Thoughts on THC (“weed”)
I add THC to the list of stimulants because it is the epitome of an anti-stimulant. The dangers of weed are often downplayed, in part because the drug is so insidious.
I have a handful of friends who had a weed problem in the past. While using it, every single one self-justified to the point it became ridiculous. After stopping, every single one was much better off mentally, physically, and with life in general, and every single one wished he/she stopped sooner.
Why is THC on a list of stimulants? Becasue stopping weed may be the only stimulant some people “need”.

I discuss THC (“weed”) in more detail here.
Noteworthy molecules stuck in pharmaceutical pipelines
What follows is a list of potentially interesting stimulant and antidepressant drugs that are either stuck in pharmaceutical pipelines or were withdrawn from the market. I have not tried any of them. Here and there I´ll add in a couple of general comments about neuropharmacology.
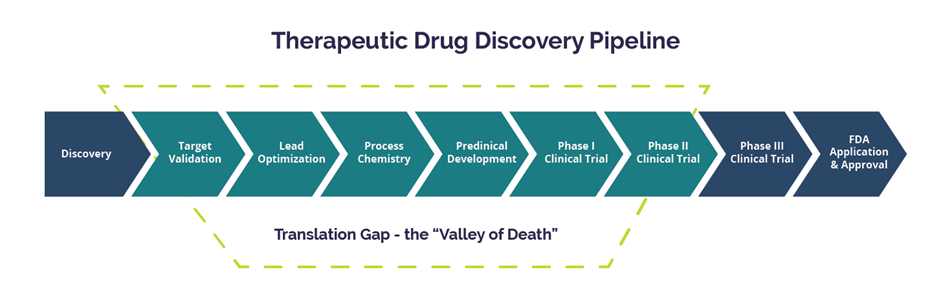
I discuss some of these molecules in more detail here.
Conclusion: On Butterflies, Upwards Spirals, and the Most Powerful Force in the Universe
Our world is a highly chaotic system. If starting conditions are even slightly altered, the trajectory and outcome can be radically different. This is called the butterfly effect.

Let’s embark on a thought experiment. Let’s clone the universe. Now you and a biological clone exist, who is identical to you down to the atomic level -identical health, mind, thoughts, and life. Then, in the parallel universe, a vicious scientist secretly injects your clone with “Agent X” every night while cloned-you is sleeping. (Note: “Agent X” is not necessarily a drug, but a catch-all term for any intervention that improves vitality, whether hormones, pharmaceutical drugs, or lifestyle changes.) The scientist then keeps track of the changes in your life versus the life of your clone.
Your clone has a little more energy right after waking up and is more optimistic about starting a new day. He needs 30min less sleep, 15 of which he then uses for the morning meditation real-you never has the time and energy for. Clone-you is also not as tired anymore. Therefore, he is able to use the afternoon lulls you experience in new and productive ways.
He has more drive to do things, procrastinates less, and is more motivated to study. Instead of browsing social media, cloned-you feels motivated enough to finally start that business you’ve always had in the back of your mind. Also, he can finally apply some of what you have read in all of these self-help books because he now has the needed energy and “presence” for it.
Thanks to the combined improvements in energy levels, drive, and motivation, your clone’s willpower increases, which allows him to make better food choices, exercise more, and improve his sleeping habits.
He has an easier time losing fat and building muscle. This causes him to look better, which makes him react with more self-confidence towards others and causes others to react with more benevolence towards him. The gains in looks (along with energy, mood, and enthusiasm) translate into a more fulfilling social life. Because of the many direct and indirect effects of “Agent X”, he is also in a better mood than you, which does not only affect his own well-being but also how much people like being around him because mood is contagious.

He has more friends and better relationships, which function as a buffer to stress, as a valuable source of feedback and wisdom, and also result in some valuable life opportunities offered to him by his social circle.
Because of his better social relationships, opportunities, and his improved ability to work hard, he also earns more money, and his wealth becomes greater than yours.
The increase in self-confidence, energy, and motivation also makes it easier for him to go out of his comfort zone more often. One time, he gets over the hump and talks to Bella, a woman he was blown away by from the first second he saw her. Down the road, she becomes his wife, which would not have happened if he did not have the courage to talk to her that day.
Having seen the evolution of their lives, if you could choose which life to have lived, would you choose your life or your clone’s?

There is no sure way to tell how the experiment will go, but for sure, your alternate futures will be different. The longer the experiment runs, the larger the differences will be. Even if cloned-you gets just a very small amount of additional value every day, over time this does add up.
And whether cloned-you is aware of it or not, he automatically reinvests this daily compounded interest anew, every single day. Day after day. 365 days a year.
For the sake of argument, let’s arbitrarily assume that cloned-you is able to grow an additional 0.1% per day on average compared to real-you. After one year, cloned-you is 45% ahead. After 5 years, 619%, and after 10 years a whopping 3840%. (Even though enticing in the simple mathematical model, this does obviously not hold up in real life. The major point is that compound interest can produce stunning results.)

While initial change is slow, down the road the small changes in energy, mood, health, etc. might lead to an upward spiral in many domains of your clone’s life. An upwards spiral real-you has little chance of catching up with.
Many fail not because their dreams do not work out but simply because they have no energy left to burn long enough for their dreams to bear fruit.
How many Bill Gates did not make it because their failing biology put a padlock in front of
their dreams? How many Elon Musks did not even start their endeavors because they did not
have the necessary vitality in the first place?
There are invisible biological shackles many people carry. Shackles that make it harder to live a life one likes. Shackles that make it harder to dream, to find purpose, and certainly much harder to have the necessary persistence, drive, energy, and health to keep working towards the things one values.
I am going to die. I do not want to waste my time. I want to become someone I and others are proud of. Discipline, commitment, having agency, being bold, taking calculated risks, doing things that move the needle, being useful to others, giving love, and finding purpose. However, I need to play long-term games. This means first and foremost putting a prime on my vitality.
As Herophilus already said, when vitality is absent, wisdom cannot reveal itself, art cannot manifest, strength cannot fight, wealth becomes useless, and intelligence cannot be applied.
